Lecture note
General organisation, cell and membrane physiology
Exam Target
Purpose. This module is the mechanism base for the rest of EDAIC Part I physiology. It links homeostasis, cell organelles, membrane permeability, transport, enzyme kinetics, and body fluid compartments to the way anaesthetic drugs, ventilation, shock, oedema, and electrolyte disorders behave in patients.
Core idea. Cells survive because the extracellular environment is regulated, membranes preserve gradients, enzymes control reaction rates, and ATP maintains ordered transport. Anaesthesia repeatedly interferes with those systems, so the exam often tests whether you can predict the consequence.
Homeostasis, feedback terms, Na+/K+-ATPase stoichiometry, osmolality versus tonicity, Km, Vmax, body water volumes, and crystalloid distribution.
How gradients, permeability, ATP, protein transporters, and effective osmoles determine cell function and compartment size.
Local anaesthetic onset, hypoxic cell swelling, hyperkalaemia, cerebral oedema, sepsis capillary leak, fluid therapy, and drug kinetics.
Revision rule. Do not learn this as a list of cell parts. Attach every fact to a mechanism: what creates a gradient, what crosses a membrane, what consumes ATP, what saturates, and what changes compartment water.
Quick check: physiology operating system
When you meet a new physiology fact, what four mechanism questions should you ask?
Show answer
Ask: which compartment is involved, what gradient exists, what membrane or protein controls movement, and whether ATP is needed to preserve the system.
Why is extracellular fluid such a central idea in anaesthesia?
Show answer
Cells exchange gases, ions, nutrients, drugs, acid-base load, and water through the extracellular environment. If ECF composition or volume is wrong, cell function fails even when the cell itself is structurally intact.
Body Organisation and the Internal Environment
What Is Physiology?
Physiology is the study of normal body function. It asks how the body works: how cells produce energy, how organs perform their specific tasks, and how organ systems cooperate to preserve life.
Physiology is the study of normal function in cells, tissues, organs, and integrated body systems.
In anaesthesia, physiology is not background decoration. It is the language used to understand patient responses to drugs, ventilation, surgical stress, blood loss, sepsis, pain, positioning, temperature change, and fluid administration.
Levels of Organisation
The body is organised in a hierarchy:
Molecules -> organelles -> cells -> tissues -> organs -> organ systems -> whole organism
| Level | Examples | Why it matters clinically |
|---|---|---|
| Molecules | Water, ions, glucose, proteins, DNA, ATP | Form receptors, channels, enzymes, membranes, and energy stores |
| Organelles | Nucleus, mitochondria, ribosomes, ER, Golgi | Run specialised intracellular tasks |
| Cells | Neurons, myocytes, hepatocytes, red cells, renal tubular cells | Basic structural and functional units |
| Tissues | Epithelial, connective, muscle, nervous | Create barriers, movement, support, and communication |
| Organs | Lung, heart, kidney, liver, brain | Perform integrated functions |
| Systems | Respiratory, cardiovascular, renal, nervous, endocrine | Preserve the internal environment |
Different cells specialise for different roles.
| Cell type | Main function |
|---|---|
| Neuron | Rapid electrical signalling |
| Skeletal muscle cell | Voluntary contraction |
| Cardiac myocyte | Rhythmic contraction |
| Red blood cell | Oxygen transport |
| Hepatocyte | Metabolism and detoxification |
| Renal tubular cell | Reabsorption and secretion |
| Endothelial cell | Vascular barrier and signalling |
| Immune cell | Defence, inflammation, phagocytosis |
Despite their differences, all cells require oxygen, nutrients, ATP, waste removal, membrane integrity, and ionic gradients.
The key idea is that organ systems are integrated. Hypotension is never only a cardiovascular issue; it affects renal perfusion, cerebral perfusion, tissue oxygen delivery, acid-base status, and drug distribution.
Internal Environment
Cells do not live directly in the external environment. They live in extracellular fluid, which supplies oxygen, glucose, electrolytes, hormones, buffer systems, temperature stability, and waste removal pathways.
| Disturbance | Cellular consequence |
|---|---|
| Hypoxaemia | Reduced oxidative phosphorylation and ATP production |
| Hyperkalaemia | Altered membrane excitability and arrhythmias |
| Hyponatraemia | Water movement into cells, especially brain cells |
| Acidosis | Altered enzyme, receptor, and channel function |
| Hypoglycaemia | Reduced cerebral energy supply |
| Hypothermia | Slowed metabolism, coagulopathy, delayed drug metabolism |
| Hyperthermia | Increased metabolic demand, enzyme dysfunction |
The body’s major systems exist largely to preserve this internal environment.
EDAIC trap: do not treat the cell as isolated. Most clinical problems in this module first disturb the extracellular fluid, then membrane gradients, then cell function.
Homeostasis and Control Systems
Homeostasis is the maintenance of a stable internal environment within limits compatible with normal cellular function.
Important regulated variables include PaO2, PaCO2, pH, temperature, blood glucose, plasma osmolality, sodium, potassium, calcium, arterial pressure, and blood volume.
| Variable | Why it matters |
|---|---|
| PaO2 | Oxygen supply for aerobic metabolism |
| PaCO2 | Ventilation, pH, cerebral blood flow |
| pH | Enzyme and protein function |
| Temperature | Enzyme activity and membrane fluidity |
| Blood glucose | Brain and cellular energy supply |
| Plasma osmolality | Water movement across membranes |
| Sodium | ECF osmolality and neuronal function |
| Potassium | Resting membrane potential and cardiac rhythm |
| Calcium | Excitation-contraction coupling, coagulation, signalling |
| Arterial pressure | Organ perfusion |
| Blood volume | Venous return and cardiac output |
Homeostasis does not mean that variables never change. It means they are regulated around a useful range. Anaesthesia often impairs these responses: opioids depress the ventilatory response to CO2, volatile agents reduce vascular tone and baroreflex responsiveness, neuromuscular blockers prevent ventilation and shivering, and neuraxial blockade prevents sympathetic vasoconstriction below the block.
Control Systems
A homeostatic control system has four basic components:
- Controlled variable - the value being regulated.
- Sensor - detects change.
- Control centre - compares the sensed value with the desired range.
- Effector - produces the response.
Example: PaCO2 regulation.
| Component | Example |
|---|---|
| Controlled variable | Arterial CO2 tension |
| Sensor | Central chemoreceptors responding to H+ changes generated by CO2 in CSF |
| Control centre | Medullary respiratory centres |
| Effector | Respiratory muscles |
| Response | Increased alveolar ventilation lowers PaCO2 |
Negative Feedback
Negative feedback is the main mechanism of physiological regulation.
Negative feedback occurs when a change in a variable triggers a response that opposes the original change and returns the variable toward its set point.
| Variable | Stimulus | Response |
|---|---|---|
| PaCO2 | Increased PaCO2 | Increased ventilation |
| Arterial pressure | Fall in MAP | Increased sympathetic tone |
| Temperature | Fall in core temperature | Vasoconstriction and shivering |
| Glucose | Rise in glucose | Insulin secretion |
| Osmolality | Rise in osmolality | ADH release and thirst |
Anaesthetic relevance: many anaesthetic drugs blunt negative feedback. A spontaneously breathing patient given opioids may not increase ventilation appropriately when CO2 rises.
Positive Feedback
Positive feedback amplifies the original change.
Useful examples include labour, haemostasis, and the action potential upstroke. Positive feedback must have a stopping mechanism. Labour ends with delivery. Clotting is limited by anticoagulant systems and fibrinolysis. Sodium channels inactivate rapidly during the action potential.
Pathological positive feedback can be dangerous. In severe haemorrhage, hypotension reduces tissue perfusion; tissue hypoxia causes acidosis and vasodilation; vasodilation worsens hypotension; and the cycle can become fatal unless interrupted.
Intrinsic, Extrinsic, and Feedforward Control
Intrinsic control is local regulation within a tissue. Active skeletal muscle produces CO2, H+, K+, adenosine, and lactate, causing local vasodilation and increased blood flow.
Extrinsic control is regulation by distant systems, mainly the nervous and endocrine systems. During haemorrhage, baroreceptor-mediated sympathetic activation affects the heart, arterioles, veins, adrenal medulla, and kidneys.
Feedforward control is anticipatory. It prepares the body before a variable has changed significantly. Preoxygenation before induction is a clinical feedforward strategy: the anaesthetist increases oxygen stores before apnoea occurs, rather than waiting for desaturation.
Quick check: homeostasis and feedback
What is the difference between homeostasis and a fixed unchanging value?
Show answer
Homeostasis keeps variables within a useful range, not at one immovable number. The body tolerates controlled variation, but responds when a variable threatens cell function.
How does negative feedback protect physiology?
Show answer
A change triggers a response that opposes the original change, such as increased PaCO2 stimulating ventilation to lower PaCO2.
Why can anaesthesia make feedback failure clinically obvious?
Show answer
Opioids blunt CO2 response, volatile agents reduce vascular tone and baroreflexes, neuromuscular blockers stop ventilation and shivering, and neuraxial blockade prevents sympathetic compensation.
EDAIC trap: homeostasis is regulated stability, not absence of change. Anaesthesia becomes dangerous when compensation is blocked or delayed.
Cell Components and Function
Basic Layout of a Cell
A typical human cell has three broad regions:
- Cell membrane - separates intracellular from extracellular fluid and controls exchange.
- Cytoplasm - intracellular fluid plus organelles.
- Nucleus - contains genetic material and regulates gene expression.
The exact appearance of cells varies. A neuron is shaped for signalling. A red blood cell is shaped for gas transport and capillary passage. A hepatocyte is packed with metabolic machinery. A skeletal muscle fibre contains organised contractile proteins. Yet all rely on membranes, ATP, proteins, enzymes, ion gradients, and controlled transport.

#f7f9f7 with no alteration to diagram lines, labels, or structures. Source link: commons.wikimedia.org/wiki/File:Animal_cell_structure_en.svg.
How to use this figure: identify nucleus, mitochondria, ER, Golgi apparatus, lysosomes, and cytoskeleton, then attach each structure to a function. For exam purposes, function is more important than visual detail.
Nucleus
The nucleus contains most of the cell’s DNA. It is enclosed by a double membrane called the nuclear envelope, which contains nuclear pores allowing controlled exchange between nucleus and cytoplasm.
Key functions include DNA storage, transcription of DNA into RNA, regulation of gene expression, cell division control, and production of ribosomal RNA in the nucleolus.
Clinical relevance: many drugs affect gene transcription indirectly through nuclear receptors, such as steroid hormones. Malignancy, inflammation, and genetic disease all involve altered gene expression.
Mitochondria
Mitochondria are the main site of aerobic ATP production. They are especially abundant in tissues with high energy demand: myocardium, skeletal muscle, renal tubular cells, hepatocytes, and neurons.
Important features include an outer membrane, inner membrane, intermembrane space, matrix, electron transport chain on the inner membrane, citric acid cycle enzymes in the matrix, mitochondrial DNA, and maternal inheritance.
Anaesthetic and ICU relevance:
- Hypoxia reduces oxidative phosphorylation.
- Cyanide poisoning blocks cytochrome oxidase, preventing oxygen use despite adequate oxygen delivery.
- Sepsis may involve mitochondrial dysfunction and impaired oxygen utilisation.
- Malignant hyperthermia and other metabolic crises show how cellular energy demand can become catastrophic.
- Red blood cells lack mitochondria and depend on glycolysis for ATP.
Endoplasmic Reticulum
The endoplasmic reticulum is a network of membranes involved in protein and lipid handling.
The rough ER has ribosomes attached. It synthesises proteins destined for secretion, membranes, or organelles. Examples include plasma proteins in hepatocytes, hormones in endocrine cells, and membrane receptors and channels.
The smooth ER lacks ribosomes. It participates in lipid synthesis, steroid synthesis, drug metabolism, and calcium storage. In muscle, specialised smooth ER is called the sarcoplasmic reticulum, which stores calcium for excitation-contraction coupling.
Clinical relevance: hepatic smooth ER participates in drug metabolism; malignant hyperthermia involves uncontrolled calcium release from the sarcoplasmic reticulum in skeletal muscle.
Ribosomes
Ribosomes translate mRNA into protein.
- Free ribosomes produce proteins used inside the cytosol.
- Bound ribosomes on rough ER produce secreted proteins, membrane proteins, and lysosomal proteins.
Protein synthesis is essential for enzyme production, receptor expression, clotting factor synthesis, and immune function.
Golgi Apparatus
The Golgi apparatus modifies, sorts, and packages proteins and lipids.
Functions include protein modification, glycosylation, sorting of proteins to membranes, lysosomes, or secretory vesicles, packaging secretory products, and formation of lysosomes.
Lysosomes and Peroxisomes
Lysosomes contain acidic digestive enzymes. They break down damaged organelles, pathogens, and macromolecules. Their functions include intracellular digestion, autophagy, recycling of cellular components, and killing engulfed microbes in immune cells.
Peroxisomes contain oxidative enzymes and catalase. They break down hydrogen peroxide, oxidise very-long-chain fatty acids, and participate in detoxification.
Oxidative stress is important in reperfusion injury, sepsis, hyperoxia, and critical illness.
Cytoskeleton
The cytoskeleton maintains cell shape and allows movement within the cell.
| Component | Main function |
|---|---|
| Microfilaments | Cell shape, contraction, movement |
| Intermediate filaments | Mechanical strength |
| Microtubules | Intracellular transport, mitotic spindle, cilia |
Clinical relevance: axonal transport in neurons depends on microtubules; cilia depend on microtubule movement; platelet shape change and immune-cell movement depend on cytoskeletal rearrangement; red blood cell deformability depends partly on membrane-cytoskeleton integrity.
Cell Junctions
| Junction | Function | Clinical relevance |
|---|---|---|
| Tight junctions | Seal between cells | Blood-brain barrier, gut, renal tubules |
| Gap junctions | Direct electrical/chemical communication | Cardiac conduction, smooth muscle coordination |
| Desmosomes | Strong mechanical attachment | Skin and myocardium |
| Adherens junctions | Cell-cell adhesion | Tissue architecture |
Tight junctions are especially important in anaesthesia because the blood-brain barrier restricts drug and solute entry into the central nervous system. Lipid-soluble drugs pass more readily than polar drugs.
Quick check: organelles and ATP failure
Why are mitochondria so clinically important in shock and hypoxia?
Show answer
They generate most aerobic ATP. Hypoxia, cyanide, sepsis, and severe shock impair ATP production, so pumps fail, gradients collapse, and cells swell or die.
Which common cell is a major exception to mitochondrial ATP production?
Show answer
The red blood cell lacks mitochondria and depends on glycolysis for ATP, which preserves oxygen carriage by preventing the cell from consuming the oxygen it transports.
What is the anaesthetic relevance of rough ER, smooth ER, and Golgi apparatus?
Show answer
Rough ER produces proteins such as channels and secreted proteins, smooth ER handles lipid synthesis, calcium storage, and drug metabolism, and the Golgi modifies and packages proteins for delivery.
EDAIC trap: organelles are tested by function. If ATP falls, membrane pumps fail; if smooth ER function changes, drug handling and calcium storage change.
Cell Membrane Structure
Core Definition
The cell membrane is a selectively permeable barrier separating intracellular fluid from extracellular fluid. It maintains different internal and external environments while allowing controlled communication and transport.
The cell membrane is a fluid phospholipid bilayer containing proteins, cholesterol, glycoproteins, and glycolipids, which separates the intracellular and extracellular compartments and regulates movement, signalling, and cell recognition.
Phospholipid Bilayer
Each phospholipid has a hydrophilic phosphate head and hydrophobic fatty-acid tails. In water, phospholipids arrange into a bilayer: hydrophilic heads face the aqueous ECF and ICF, while hydrophobic tails face inward, forming a lipid core.
This hydrophobic core is the reason membranes are selectively permeable. It allows lipid-soluble substances to pass easily but restricts charged and polar substances.

#f7f9f7 with no alteration to diagram lines, labels, or structures. Source link: commons.wikimedia.org/wiki/File:Cell_membrane_detailed_diagram_en.svg.
How to use this figure: connect visible structure to function. The lipid bilayer explains selective permeability, proteins explain transport and signalling, cholesterol modifies fluidity, and carbohydrate chains support recognition and barrier behaviour.
Substances that cross easily include O2, CO2, nitrogen, steroid hormones, volatile anaesthetics, many lipid-soluble IV drugs, and unionised weak acids or bases.
Substances that cross poorly without channels or carriers include Na+, K+, Ca2+, Cl-, glucose, amino acids, proteins, and highly ionised drugs.
Fluid Mosaic Model
The membrane is not a rigid wall. It behaves as a two-dimensional fluid with proteins floating within or attached to it.
The mosaic consists of phospholipids, cholesterol, transmembrane proteins, peripheral proteins, glycoproteins, and glycolipids. This fluidity allows cells to change shape, vesicles to fuse with membranes, receptors to move within the membrane, and red blood cells to deform through capillaries.
Membrane Cholesterol
Cholesterol modulates membrane fluidity and stability. At high temperature, cholesterol restrains excessive fluidity. At low temperature, it prevents the membrane becoming too rigid. It also reduces permeability to water and small polar molecules.
Anaesthetic relevance: membrane fluidity affects receptor and channel behaviour, although modern anaesthetic mechanisms are understood mainly through specific protein targets rather than a simple lipid theory.
Membrane Proteins
| Protein type | Function | Example |
|---|---|---|
| Ion channel | Rapid selective ion movement | Voltage-gated Na+ channel |
| Carrier | Transport by conformational change | GLUT transporter |
| Pump | ATP-dependent active transport | Na+/K+-ATPase |
| Receptor | Signal detection | GABA-A receptor, beta receptor |
| Enzyme | Catalysis at membrane surface | Adenylyl cyclase |
| Adhesion molecule | Cell attachment | Integrins, cadherins |
Glycocalyx and Cell Recognition
Carbohydrate chains on glycoproteins and glycolipids form part of the cell surface glycocalyx.
Functions include cell recognition, immune identification, adhesion, endothelial barrier function, and mechanotransduction in blood vessels. In critical illness and sepsis, endothelial glycocalyx injury contributes to capillary leak and oedema.
Membrane Specialisation
| Tissue | Specialisation | Purpose |
|---|---|---|
| Neuron | Voltage-gated channels | Action potentials |
| Skeletal muscle | Neuromuscular junction receptors | Transmission from nerve to muscle |
| Renal tubule | Polarised transporters | Directional reabsorption/secretion |
| Brain capillary endothelium | Tight junctions | Blood-brain barrier |
| Intestinal epithelium | Microvilli and transporters | Absorption |
| Cardiac myocytes | Gap junctions | Electrical coupling |
EDAIC trap: lipid solubility helps a molecule enter the membrane, but charged ions and polar drugs still need channels, carriers, pumps, or a unionised fraction.
Membrane Transport Mechanisms
Overview
Membrane transport determines how gases, ions, nutrients, water, drugs, hormones, and waste products move between compartments.
| Transport type | Energy required? | Direction |
|---|---|---|
| Simple diffusion | No | Down gradient |
| Facilitated diffusion | No | Down gradient |
| Osmosis | No direct ATP | Water follows osmotic gradient |
| Filtration | No direct ATP | Driven by pressure gradient |
| Primary active transport | Yes, ATP directly | Against gradient |
| Secondary active transport | Uses stored ion gradient | Often against gradient |
| Endocytosis/exocytosis | Yes | Vesicular transport |
Simple Diffusion
Simple diffusion is movement of molecules down a concentration or partial-pressure gradient without energy and without a carrier.
Rate of diffusion increases with a larger concentration gradient, greater lipid solubility, smaller molecular size, larger membrane surface area, thinner membrane, and higher temperature.
Clinical examples include O2 and CO2 movement across the alveolar-capillary membrane, volatile anaesthetic movement between alveoli, blood, and brain, and diffusion of lipid-soluble drugs across the blood-brain barrier.
Fick’s Law - Concept Only
Rate of diffusion is proportional to:
Area x concentration gradient x diffusion coefficient / thickness
For this module, remember:
- more area means faster diffusion,
- larger gradient means faster diffusion,
- thinner barrier means faster diffusion,
- higher lipid solubility and smaller size mean faster diffusion.
Facilitated Diffusion
Facilitated diffusion is movement down a concentration gradient through a specific protein channel or carrier. It does not require ATP.
Key features: passive, down gradient, specific, saturable, and competitively inhibitable.

#f7f9f7 with no alteration to diagram lines, labels, or structures. Source link: commons.wikimedia.org/wiki/File:Scheme_facilitated_diffusion_in_cell_membrane-en.svg.
How to use this figure: the transport protein is the key. Facilitated diffusion is passive and down-gradient, but it is selective and saturable because transporter number is finite.
Examples include GLUT transporters for glucose, amino acid transporters, and ion movement through open channels.
Ion Channels
Ion channels are protein pores allowing selective ion movement down electrochemical gradients.
| Channel type | Opens in response to | Example |
|---|---|---|
| Leak channel | Usually open | K+ leak channels |
| Voltage-gated | Membrane potential change | Voltage-gated Na+ channel |
| Ligand-gated | Chemical binding | Nicotinic ACh receptor, GABA-A receptor |
| Mechanically gated | Stretch or pressure | Baroreceptor/stretch channels |
Important anaesthetic examples:
- Local anaesthetics block voltage-gated sodium channels from the intracellular side.
- Non-depolarising neuromuscular blockers antagonise nicotinic acetylcholine receptors.
- Suxamethonium activates nicotinic receptors and causes persistent depolarisation.
- Many sedatives and anaesthetics enhance GABA-A chloride-channel activity.
Ion channels are fast. They are ideal for action potentials, synaptic transmission, cardiac conduction, skeletal muscle contraction, and smooth muscle tone.
Osmosis
Osmosis is the movement of water across a semipermeable membrane from a region of lower solute concentration to a region of higher solute concentration. More precisely, water moves toward the compartment with higher effective osmotic pressure.

#f7f9f7 with no alteration to diagram lines, labels, or structures. Source link: commons.wikimedia.org/wiki/File:Osmotic_pressure_on_blood_cells_diagram.svg.
Abbreviations shown: H2O = water.
How to use this figure: hypotonic extracellular fluid drives water into cells, hypertonic extracellular fluid draws water out, and isotonic extracellular fluid preserves cell volume. This is the logic behind hyponatraemic cerebral oedema and hypertonic saline therapy.
Osmolality is osmoles per kg of solvent. Osmolarity is osmoles per litre of solution. In clinical practice, osmolality is preferred because it is less affected by temperature and volume changes.
Approximate plasma osmolality:
2 x Na+ + glucose + urea, with all measured in mmol/L.
Normal plasma osmolality is approximately 275-295 mOsm/kg.
Tonicity refers to the effect of a solution on cell volume. It depends on effective osmoles that do not freely cross the cell membrane.
| Solution type | Effect on cells |
|---|---|
| Isotonic | No major change in cell volume |
| Hypotonic | Water enters cells; cells swell |
| Hypertonic | Water leaves cells; cells shrink |
Urea contributes to measured osmolality but crosses many membranes relatively easily, so it is less effective at sustaining osmotic gradients across many cells. Sodium is the main determinant of extracellular tonicity.
Clinical examples:
- Hyponatraemia lowers extracellular tonicity. Water moves into cells, especially brain cells.
- Hypernatraemia raises extracellular tonicity. Water leaves cells and brain cells shrink.
- Mannitol and hypertonic saline reduce cerebral oedema by increasing plasma tonicity, drawing water from brain tissue into the intravascular compartment if the blood-brain barrier is sufficiently intact.
Filtration
Filtration is movement of fluid across a membrane driven by a pressure gradient.
Examples include glomerular filtration in the kidney, capillary fluid movement, and ultrafiltration during renal replacement therapy.
Filtration is influenced by hydrostatic pressure, oncotic pressure, membrane permeability, surface area, and integrity of the endothelial glycocalyx.
Primary Active Transport
Primary active transport uses ATP directly to move substances against electrochemical gradients.
Na+/K+-ATPase is one of the most important pumps in physiology. It moves:
- 3 Na+ out of the cell,
- 2 K+ into the cell,
- using 1 ATP.

#f7f9f7 with no alteration to diagram lines, labels, or structures. Source link: commons.wikimedia.org/wiki/File:Scheme_sodium-potassium_pump-en.svg.
Abbreviations shown: Na+ = sodium ion; K+ = potassium ion; ATP = adenosine triphosphate; ADP = adenosine diphosphate; Pi = inorganic phosphate.
How to use this figure: fix the direction in memory. Na+/K+-ATPase uses ATP to move three sodium ions out and two potassium ions in; false statements commonly reverse the direction or remove ATP from the mechanism.
Main functions:
- maintains low intracellular sodium,
- maintains high intracellular potassium,
- helps maintain resting membrane potential,
- controls cell volume,
- provides the sodium gradient used for secondary active transport.
Why it is electrogenic: 3 positive charges leave for every 2 positive charges entering, producing a small net outward positive current.
Clinical relevance:
- Hypoxia reduces ATP, causing Na+/K+-ATPase failure.
- Intracellular sodium rises.
- Water enters cells osmotically.
- Cells swell: this is cytotoxic oedema.
- Hyperkalaemia alters membrane potential and can cause arrhythmias.
- Digoxin inhibits Na+/K+-ATPase in cardiac myocytes, indirectly increasing intracellular calcium and contractility.
Other important pumps include Ca2+-ATPase, which maintains low cytosolic calcium, and H+/K+-ATPase in gastric parietal cells, which is inhibited by proton pump inhibitors.
Secondary Active Transport
Secondary active transport does not use ATP directly at the transporter. It uses an ion gradient created by primary active transport.
| Type | Direction of movement |
|---|---|
| Symport / co-transport | Two substances move in the same direction |
| Antiport / counter-transport | Substances move in opposite directions |
Examples include Na+/glucose co-transport in renal tubule and gut, Na+/Ca2+ exchange in cardiac cells, and Na+/H+ exchange in acid-base regulation.
Endocytosis
Endocytosis brings material into the cell by membrane invagination and vesicle formation. It requires energy.
| Type | What is taken in | Example |
|---|---|---|
| Phagocytosis | Large particles, bacteria, debris | Neutrophils and macrophages engulf bacteria |
| Pinocytosis | Fluid and small solutes | Non-specific fluid uptake |
| Receptor-mediated endocytosis | Specific ligand-receptor complexes | LDL cholesterol, iron-transferrin uptake |
Exocytosis
Exocytosis releases material from cells when intracellular vesicles fuse with the cell membrane.
Examples include neurotransmitter release, hormone secretion, enzyme secretion, and inflammatory mediator release.
At nerve terminals, calcium entry triggers vesicle fusion and neurotransmitter release. Botulinum toxin prevents acetylcholine release by interfering with vesicle fusion machinery.
Transport Mechanisms Compared
How to use this table: first decide whether movement is down a gradient or against it, then ask whether ATP is used directly. That sequence prevents most exam mistakes.
| Mechanism | ATP? | Protein required? | Direction | Saturable? | Example |
|---|---|---|---|---|---|
| Simple diffusion | No | No | Down gradient | No | O2, CO2, volatile agents |
| Facilitated diffusion | No | Yes | Down gradient | Yes | GLUT transport |
| Ion channel | No | Yes | Down electrochemical gradient | Usually not like carriers | Na+ channel |
| Osmosis | No direct ATP | Sometimes aquaporins | Water toward effective osmoles | No | Water shift in hyponatraemia |
| Filtration | No direct ATP | Barrier-dependent | Pressure gradient | No | Glomerular filtration |
| Primary active transport | Yes | Pump | Against gradient | Yes | Na+/K+-ATPase |
| Secondary active transport | Indirect | Co-transporter/exchanger | Uses stored gradient | Yes | Na+/glucose co-transport |
| Endocytosis | Yes | Vesicle machinery | Into cell | Yes | Phagocytosis |
| Exocytosis | Yes | Vesicle machinery | Out of cell | Yes | ACh release |
Quick check: membrane transport
What separates simple diffusion from facilitated diffusion?
Show answer
Both move down a gradient without ATP. Simple diffusion crosses the lipid bilayer directly, while facilitated diffusion uses a specific channel or carrier and is therefore selective and saturable.
How do primary and secondary active transport differ?
Show answer
Primary active transport directly uses ATP to move solute against a gradient. Secondary active transport uses a stored ion gradient, commonly sodium, to drive another solute uphill.
What happens when Na+/K+-ATPase fails during severe hypoxia?
Show answer
Sodium accumulates inside cells, potassium gradients fall, water follows sodium into cells, and cytotoxic oedema develops. In brain injury this can raise intracranial pressure.
EDAIC trap: facilitated diffusion is still passive. Protein involvement alone does not make a process active transport.
Enzymes
Definition
An enzyme is a biological catalyst, usually a protein, that increases the rate of a chemical reaction without being consumed.
An enzyme is a biological catalyst that lowers activation energy and increases reaction rate without being permanently altered by the reaction.
Enzymes make life possible because many biochemical reactions would otherwise be too slow at body temperature.
Enzyme Structure and the Active Site
Enzymes have a three-dimensional structure containing an active site. The substrate binds to the active site to form an enzyme-substrate complex. The reaction occurs, product is released, and the enzyme is available again.
Basic sequence:
E + S <-> ES -> E + P
Enzyme specificity arises because the active site has a particular shape, charge distribution, and chemical environment.
Activation Energy
Chemical reactions require an energy barrier to be overcome. This is activation energy.
Enzymes lower activation energy by bringing substrates together, orientating substrates correctly, stabilising the transition state, altering local pH or charge, and sometimes forming temporary covalent intermediates.
They do not change the final equilibrium of a reaction; they allow equilibrium to be reached faster.
Factors Affecting Enzyme Activity
| Factor | Effect | Clinical relevance |
|---|---|---|
| Temperature | Rate rises until denaturation | Hypothermia slows metabolism; hyperthermia impairs protein function |
| pH | Each enzyme has an optimal pH | Acidosis alters contractility, catecholamine response, potassium, drug ionisation |
| Substrate concentration | Low substrate: rate rises; high substrate: saturation | Explains first-order and zero-order kinetics |
| Enzyme concentration | More enzyme increases capacity if substrate is available | Enzyme deficiency or induction changes drug effect |
| Cofactors/coenzymes | Some enzymes require helpers | Mg2+, Zn2+, Fe2+, vitamins, NAD+, FAD, coenzyme A |
Michaelis-Menten Kinetics
Many enzymes follow Michaelis-Menten kinetics:
v = Vmax x [S] / (Km + [S])
where v is reaction velocity, Vmax is maximum reaction velocity when the enzyme is saturated, [S] is substrate concentration, and Km is the substrate concentration at which reaction velocity is half of Vmax.

#f7f9f7 with no alteration to graph lines, labels, or data. Source link: commons.wikimedia.org/wiki/File:Michaelis-Menten_saturation_curve_of_an_enzyme_reaction.svg.
Abbreviations shown: Vmax = maximum reaction velocity; Km = substrate concentration at half Vmax.
How to use this figure: below half Vmax, reaction velocity is substrate-sensitive; near Vmax, enzyme saturation limits further increase in velocity. Use this curve to distinguish capacity limitation from affinity.
Km is often used as an inverse marker of enzyme affinity:
- Low Km: half-maximal velocity at low substrate concentration, suggesting high affinity.
- High Km: higher substrate concentration is needed, suggesting lower affinity.
At low substrate concentration, the rate is proportional to substrate concentration: first-order kinetics. At high substrate concentration, the enzyme is saturated and the rate approaches Vmax: zero-order kinetics.
Clinical examples of saturable metabolism include ethanol, phenytoin, and high-dose salicylates. The principle matters because saturation can make drug concentration rise disproportionately with dose.
Enzyme Inhibition
| Inhibition type | Site/mechanism | Km | Vmax | Can increasing substrate overcome it? |
|---|---|---|---|---|
| Competitive | Active site competition | Increased | Same | Yes |
| Non-competitive | Reduces enzyme activity away from active site | Same or variable | Decreased | No |
| Uncompetitive | Binds enzyme-substrate complex | Decreased | Decreased | No |
| Irreversible | Permanently inactivates enzyme | Variable | Decreased | No, new enzyme needed |
Competitive inhibition increases Km but leaves Vmax unchanged. Neostigmine competes with acetylcholine at acetylcholinesterase, increasing acetylcholine at the neuromuscular junction.
Non-competitive inhibition reduces Vmax and cannot be fully overcome by increasing substrate. Irreversible inhibition permanently inactivates enzyme molecules; aspirin irreversibly inhibits cyclo-oxygenase in platelets.
Enzymes of Anaesthetic Importance
| Enzyme | Relevance |
|---|---|
| Plasma cholinesterase / pseudocholinesterase | Metabolism of suxamethonium and mivacurium; deficiency causes prolonged paralysis |
| Acetylcholinesterase | Terminates acetylcholine action at synapses and NMJ; inhibited by neostigmine and organophosphates |
| CYP450 enzymes | Hepatic drug metabolism; induction and inhibition cause drug interactions |
| Esterases | Metabolism of remifentanil and ester local anaesthetics |
| Carbonic anhydrase | CO2/HCO3- handling; CSF production; inhibited by acetazolamide |
| COMT and MAO | Catecholamine metabolism |
| HMG-CoA reductase | Cholesterol synthesis; statin target |
| Cyclo-oxygenase | Prostaglandin synthesis; NSAID target |
Exam trap: plasma cholinesterase deficiency causes prolonged suxamethonium paralysis because the drug is not metabolised normally. Malignant hyperthermia is a skeletal muscle calcium-handling disorder triggered by volatile agents and suxamethonium in susceptible patients.
Quick check: enzyme kinetics
What do Km and Vmax tell you?
Show answer
Km is the substrate concentration at half Vmax and is often used as an inverse marker of affinity. Vmax is the maximum reaction velocity when the enzyme system is saturated.
What does competitive inhibition do to Km and Vmax?
Show answer
It increases apparent Km because more substrate is needed to reach half Vmax, but Vmax is unchanged if enough substrate is present.
Why do saturable drug processes matter clinically?
Show answer
Once the enzyme capacity is near Vmax, small dose increases can cause disproportionate concentration increases, as with phenytoin, ethanol, and high-dose salicylate.
EDAIC trap: Km and Vmax describe behaviour, not drug names. Competitive inhibition mainly changes apparent Km; non-competitive inhibition lowers Vmax.
Body Fluid Compartments
Why Compartments Matter
Anaesthetists give fluids, blood, electrolytes, osmotic agents, and drugs into compartments that are not static containers. Fluid moves according to hydrostatic pressure, oncotic pressure, osmotic gradients, endothelial permeability, membrane transport, and renal regulation.
This answers questions such as: Where does 1 L of saline go? Why does 5% dextrose behave like free water? Why does hypertonic saline reduce cerebral oedema? Why does sepsis cause oedema despite low circulating volume?
Total Body Water
In a typical 70 kg adult male:
- Total body water is approximately 60% of body weight.
- 60% of 70 kg = 42 L.
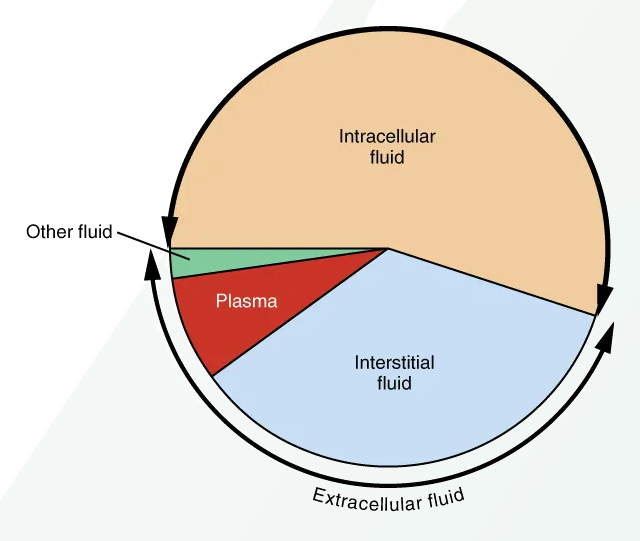
#f7f9f7; original diagram content otherwise unchanged. Source link: openstax.org/books/anatomy-and-physiology-2e/pages/26-1-body-fluids-and-fluid-compartments.
How to use this figure: anchor the numbers for a 70 kg adult male: 42 L total body water, 28 L intracellular, 14 L extracellular, and about 3-3.5 L plasma. These values drive fluid distribution questions.
| Compartment | % body weight | Approximate volume in 70 kg male |
|---|---|---|
| Total body water | 60% | 42 L |
| Intracellular fluid | 40% | 28 L |
| Extracellular fluid | 20% | 14 L |
| Interstitial fluid | 15% | 10-10.5 L |
| Plasma | 5% | 3-3.5 L |
| Transcellular fluid | <1-2% | ~1 L |
Another way to remember it:
- Two-thirds of total body water is intracellular.
- One-third of total body water is extracellular.
- Three-quarters of ECF is interstitial.
- One-quarter of ECF is plasma.
So, in a 70 kg man:
42 L TBW = 28 L ICF + 14 L ECF
14 L ECF = about 10.5 L interstitial + 3.5 L plasma
Variation With Age, Sex, and Body Composition
| Group | Total body water |
|---|---|
| Adult male | ~60% body weight |
| Adult female | ~50-55% body weight |
| Elderly | Lower than young adults |
| Obesity | Lower percentage because fat contains less water |
| Neonate | ~75-85% body weight |
| Premature neonate | Even higher ECF fraction |
Clinical relevance:
- Neonates have high total body water and high extracellular fluid, so they are vulnerable to rapid fluid loss and electrolyte disturbance.
- Elderly patients have less total body water and often reduced renal reserve, so dehydration and drug concentration changes occur more easily.
- Obese patients have lower water percentage relative to body weight, affecting dosing and distribution of hydrophilic drugs.
Intracellular and Extracellular Composition
| Compartment | Main cation | Main anions |
|---|---|---|
| Intracellular fluid | K+, Mg2+ | Phosphate, proteins |
| Extracellular fluid | Na+ | Cl-, HCO3- |
| Plasma | Na+ | Cl-, HCO3-, proteins |
| Interstitial fluid | Na+ | Cl-, HCO3-, low protein |
| Variable | Approximate value |
|---|---|
| Extracellular Na+ | 135-145 mmol/L |
| Intracellular Na+ | ~10-15 mmol/L |
| Extracellular K+ | 3.5-5.0 mmol/L |
| Intracellular K+ | ~140 mmol/L |
| Plasma osmolality | 275-295 mOsm/kg |
| Plasma albumin | 35-50 g/L |
The sodium gradient is essential for osmolality, extracellular volume, action potentials, and secondary transport. The potassium gradient is essential for resting membrane potential.
Indicator Dilution Method
The volume of a body fluid compartment can be estimated using indicator dilution:
Volume = amount of indicator administered / concentration after equilibration
The indicator must distribute only in the compartment being measured, not be metabolised rapidly, not be excreted significantly before measurement, not alter the compartment volume, and be safe and measurable.
| Compartment | Example indicator |
|---|---|
| Total body water | Deuterium oxide, tritiated water, antipyrine |
| Extracellular fluid | Inulin, mannitol, thiosulfate, sulfate |
| Plasma volume | Radio-labelled albumin, Evans blue dye |
| Intracellular fluid | Calculated: TBW - ECF |
| Interstitial fluid | Calculated: ECF - plasma volume |
Example: if 10 mg of indicator is injected and, after equilibration, concentration is 2 mg/L, then volume = 10 / 2 = 5 L.
Fluid Distribution After IV Administration
| Infusion | Main distribution after equilibration | Clinical message |
|---|---|---|
| 1 L 0.9% saline or balanced crystalloid | ECF: ~250 mL plasma, ~750 mL interstitial | Good for ECF expansion, limited plasma retention |
| 1 L 5% dextrose | TBW: ~667 mL ICF, ~333 mL ECF, ~83 mL plasma | Behaves like free water after glucose metabolism |
| Colloid | Intended intravascular retention | Advantage reduced by capillary leak |
| Hypertonic saline | Increases ECF tonicity and draws water out of cells | Small-volume expansion and cerebral oedema therapy |
This is why 5% dextrose is poor for intravascular resuscitation and can worsen hyponatraemia.
Capillary and Interstitial Fluid Movement
Fluid movement between plasma and interstitium depends on capillary hydrostatic pressure, interstitial hydrostatic pressure, plasma oncotic pressure, interstitial oncotic pressure, capillary permeability, endothelial glycocalyx, and lymphatic drainage.
Traditional Starling forces remain useful, but the endothelial glycocalyx is now recognised as a major determinant of vascular barrier function.
| Oedema mechanism | Example |
|---|---|
| Increased capillary hydrostatic pressure | Heart failure, venous obstruction |
| Reduced plasma oncotic pressure | Hypoalbuminaemia, liver disease, nephrotic syndrome |
| Increased permeability | Sepsis, burns, inflammation, anaphylaxis |
| Lymphatic obstruction | Malignancy, surgery, radiotherapy |
| Sodium and water retention | Renal failure, heart failure |
Quick check: compartments and IV fluids
In a 70 kg adult, what are the high-yield body water volumes?
Show answer
Total body water is about 42 L. Intracellular fluid is about 28 L. Extracellular fluid is about 14 L, divided into about 3 to 3.5 L plasma and about 10 to 10.5 L interstitial fluid.
Where does 1 L of isotonic crystalloid mostly go after equilibration?
Show answer
It remains in the extracellular compartment: roughly 250 mL in plasma and 750 mL in interstitial fluid, so plasma expansion is limited.
Why is 5% dextrose poor for intravascular resuscitation?
Show answer
After glucose is metabolised it behaves mainly like free water, distributing through total body water. Only a small fraction remains intravascular, and it can worsen hyponatraemia.
EDAIC trap: fluid choice is compartment physiology. Isotonic crystalloid expands ECF, dextrose becomes free water, and effective osmoles determine water movement across cells.
Clinical Integration
Why Propofol Works Quickly
Propofol is highly lipid soluble. After IV injection it rapidly reaches the brain because the brain has high blood flow and propofol crosses lipid membranes readily. Its early offset after a bolus is mainly due to redistribution from brain to muscle and fat, not immediate metabolism.
Key principles: lipid solubility, blood flow, membrane diffusion, protein binding, and redistribution.
Why Local Anaesthetic Onset Depends on pKa
Local anaesthetics are weak bases. They exist in equilibrium between unionised and ionised forms.
- Unionised form crosses the nerve membrane.
- Ionised form blocks the sodium channel from the intracellular side.
If pKa is closer to physiological pH, more drug is unionised and onset is faster. In infected acidic tissue, more drug becomes ionised outside the nerve, less crosses the membrane, and block is less effective.
Why Hypoxia Causes Cell Swelling
Hypoxia reduces oxidative phosphorylation and ATP production. Na+/K+-ATPase cannot maintain sodium gradients. Sodium accumulates inside cells. Water follows osmotically. Cells swell. This is cytotoxic oedema.
In the brain, cytotoxic oedema can raise intracranial pressure and worsen cerebral perfusion.
Why Sepsis Causes Oedema Despite Low Effective Circulating Volume
Sepsis causes inflammatory endothelial injury, glycocalyx damage, vasodilation, and increased capillary permeability. Fluid and proteins move into the interstitial space. The patient may be oedematous but still have inadequate effective circulating volume and impaired tissue perfusion.
This explains why fluid therapy in sepsis must be reassessed repeatedly rather than given blindly.
Why Suxamethonium Can Be Dangerous in Some Patients
Suxamethonium depolarises the neuromuscular junction. In normal muscle, potassium efflux is usually small. In denervation, burns, prolonged immobilisation, spinal cord injury, and some neuromuscular diseases, extrajunctional acetylcholine receptors proliferate. Suxamethonium can then cause massive potassium efflux and life-threatening hyperkalaemia.
This is a membrane receptor and ion-gradient problem.
Why Plasma Cholinesterase Deficiency Prolongs Paralysis
Suxamethonium is normally rapidly hydrolysed by plasma cholinesterase. If enzyme activity is reduced genetically or acquired, suxamethonium persists longer, causing prolonged neuromuscular blockade and apnoea.
This is an enzyme kinetics and drug metabolism problem, not a primary nerve or lung problem.
Exam Values and Definitions
Values to Memorise
| Item | Value |
|---|---|
| Total body water, adult male | ~60% body weight |
| TBW in 70 kg man | ~42 L |
| ICF | ~2/3 TBW = 28 L |
| ECF | ~1/3 TBW = 14 L |
| Plasma volume | ~3-3.5 L |
| Interstitial fluid | ~10-10.5 L |
| Transcellular fluid | ~1 L |
| Plasma Na+ | 135-145 mmol/L |
| Plasma K+ | 3.5-5.0 mmol/L |
| Intracellular K+ | ~140 mmol/L |
| Plasma osmolality | 275-295 mOsm/kg |
| Adult blood volume | ~70 mL/kg |
| pH | 7.35-7.45 |
| Core temperature | ~37°C |
Definitions
| Term | Definition |
|---|---|
| Homeostasis | Maintenance of a stable internal environment within limits compatible with normal cell function |
| Negative feedback | A control process in which a change triggers a response that opposes the original change |
| Positive feedback | A process in which a change triggers responses that amplify the original change |
| Cell membrane | A selectively permeable phospholipid bilayer containing proteins and other molecules that separates ICF from ECF and regulates transport and signalling |
| Simple diffusion | Passive movement down a concentration or partial-pressure gradient without a carrier or energy |
| Facilitated diffusion | Passive movement down a gradient via a specific membrane protein |
| Primary active transport | ATP-dependent movement against an electrochemical gradient |
| Secondary active transport | Movement using energy stored in an ion gradient created by primary active transport |
| Osmosis | Movement of water across a semipermeable membrane toward higher effective solute concentration |
| Enzyme | Biological catalyst that increases reaction rate by lowering activation energy |
| Km | Substrate concentration at which reaction velocity is half of Vmax |
| Vmax | Maximum reaction velocity when enzyme is saturated |
Exam Traps
- Homeostasis is not “no change.” It is controlled change within acceptable limits.
- Osmolality and tonicity are not identical. Tonicity depends on effective osmoles.
- 5% dextrose is not a resuscitation fluid. After glucose metabolism it behaves like free water.
- Crystalloid does not stay intravascular. Only about one-quarter of isotonic crystalloid remains in plasma after distribution.
- Unionised drug crosses membranes; ionised local anaesthetic blocks the sodium channel. Both forms matter.
- Facilitated diffusion is passive. It uses proteins but not ATP.
- Primary active transport directly uses ATP. Secondary active transport uses stored ion gradients.
- Competitive inhibition increases Km but does not reduce Vmax.
- Non-competitive inhibition reduces Vmax.
- Plasma cholinesterase deficiency causes prolonged suxamethonium paralysis; malignant hyperthermia is a calcium-handling crisis.
End-of-Module Summary
The body is organised from molecules to cells, tissues, organs, and organ systems. Physiology is the study of how these systems function and integrate. The immediate environment of cells is the extracellular fluid, and homeostasis preserves this environment through negative feedback, positive feedback, intrinsic control, extrinsic control, and feedforward mechanisms.
Cells contain specialised organelles. The nucleus stores genetic information. Mitochondria produce ATP. The endoplasmic reticulum synthesises proteins and lipids and stores calcium. The Golgi apparatus modifies and packages proteins. Lysosomes digest material. The cytoskeleton maintains structure and transport.
The cell membrane is a fluid phospholipid bilayer containing cholesterol, proteins, glycoproteins, and glycolipids. Its hydrophobic core permits lipid-soluble molecules to pass and restricts polar or charged substances unless channels, carriers, or pumps are present.
Membrane transport may be passive, active, osmotic, pressure-driven, or vesicular. Simple diffusion moves lipid-soluble molecules down gradients. Facilitated diffusion uses proteins but no ATP. Primary active transport directly uses ATP, with Na+/K+-ATPase as the key example. Secondary active transport uses gradients created by primary transport. Endocytosis and exocytosis move larger substances by vesicles.
Enzymes are biological catalysts. Michaelis-Menten kinetics describe the relation between substrate concentration and reaction rate. Km is the substrate concentration at half Vmax. Competitive inhibitors increase Km without changing Vmax; non-competitive inhibitors reduce Vmax.
Total body water in a 70 kg adult male is about 42 L: 28 L intracellular and 14 L extracellular. The extracellular compartment contains interstitial fluid, plasma, and transcellular fluid. Fluid therapy makes sense only when these compartments are understood.
Anaesthetic drugs, oxygen, carbon dioxide, electrolytes, water, and hormones all act through cells, membranes, enzymes, and compartments. Mastering this module makes the rest of physiology easier.