Lecture note
Genetics and Basic Biochemistry for Anaesthetists
Exam Target
Purpose. Module 1.2 should not be a detached genetics chapter. For EDAIC Part I, the useful aim is to understand how inherited variation, protein structure, enzyme pathways, and metabolic stress explain anaesthetic hazards that may be silent until drug exposure.
Core idea. DNA determines RNA, RNA determines protein, protein determines enzyme/channel/receptor function, and altered protein function changes anaesthetic risk. Porphyria, malignant hyperthermia, and pseudocholinesterase deficiency are the key clinical anchors.
Gene, allele, genotype, phenotype, penetrance, expressivity, codon, mutation, polymorphism, Km-style enzyme thinking, and inheritance patterns.
How DNA sequence changes alter protein structure, enzyme activity, receptor/channel behaviour, metabolism, and drug response.
Porphyria drug safety, malignant hyperthermia triggers and dantrolene, pseudocholinesterase deficiency, pharmacogenetic variability, and mitochondrial vulnerability.
Revision rule. Do not memorise genetics as vocabulary alone. Attach every term to an anaesthetic consequence: inheritance risk, altered drug metabolism, altered receptor response, or metabolic crisis.
Quick check: genetics operating frame
What is the central clinical question when genetics appears in anaesthesia?
Reveal answer
Ask whether an inherited variant changes a protein enough to alter physiology, drug handling, or susceptibility to an anaesthetic emergency.
Why is vocabulary alone a weak way to learn this module?
Reveal answer
The terms matter because they predict inheritance, expression, penetrance, drug response, and perioperative risk.
What makes a genetic disorder anaesthesia-relevant?
Reveal answer
It changes enzyme activity, receptor or ion-channel function, muscle calcium handling, haem synthesis, mitochondrial reserve, or drug metabolism.
EDAIC trap: do not learn genetic terms as isolated vocabulary. The exam usually asks what a molecular change does to a protein, enzyme, receptor, ion channel, or inherited anaesthetic risk.
DNA, Genes, and Chromosomes
DNA: The Storage Molecule
For anaesthetists, DNA matters because it stores the instructions for proteins that become receptors, ion channels, enzymes, transporters, contractile proteins, and metabolic pathways. A clinically silent DNA variant may become important only when a drug or physiological stress challenges that protein system.
DNA is made from repeating units called nucleotides. Each nucleotide contains a deoxyribose sugar, a phosphate group, and a nitrogenous base.
How to use this table: first separate purines from pyrimidines, then remember that RNA replaces thymine with uracil.
| Base | Abbreviation | Type |
|---|---|---|
| Adenine | A | Purine |
| Guanine | G | Purine |
| Cytosine | C | Pyrimidine |
| Thymine | T | Pyrimidine |
DNA is a double helix made of two antiparallel strands. The sugar-phosphate backbone is on the outside, and the bases face inward.
Base pairing is specific:
- Adenine pairs with thymine: A-T.
- Guanine pairs with cytosine: G-C.
A-T has two hydrogen bonds. G-C has three hydrogen bonds. This matters because GC-rich DNA regions are more stable and require more energy to separate.
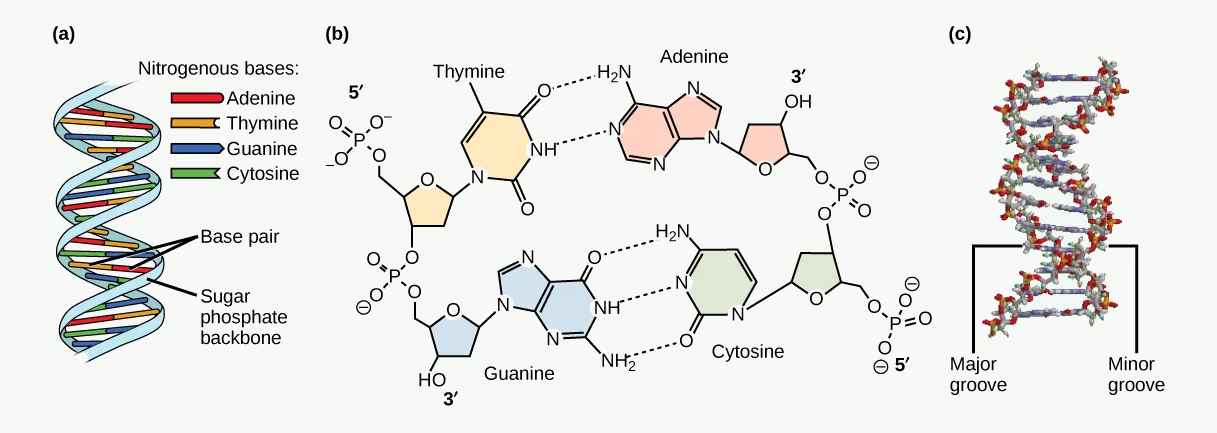
#f7f9f7; original diagram content otherwise unchanged. Source link: openstax.org/books/biology-2e/pages/14-2-dna-structure-and-sequencing.
Abbreviations shown: 5' = five-prime end; 3' = three-prime end.
How to use this figure: fix the base-pairing rules and strand direction. Complementary pairing explains replication, transcription, mutation detection, and why GC-rich regions are more thermally stable.
Why Complementary Base Pairing Matters
Complementary base pairing explains accurate DNA replication, transcription of DNA into RNA, repair of damaged DNA, polymerase chain reaction in genetic testing, and detection of mutations.
If one strand is:
A T G C C A
The complementary strand is:
T A C G G T
This is the molecular basis of heredity: each strand can act as a template for the other.
DNA Packaging
A human cell contains a very long DNA molecule, but it must fit inside the nucleus. DNA is packaged by winding around proteins called histones, forming nucleosomes. Nucleosomes coil and fold further to form chromatin. During cell division, chromatin condenses into visible chromosomes.
Human somatic cells have:
- 46 chromosomes,
- arranged as 23 pairs,
- 22 pairs of autosomes,
- 1 pair of sex chromosomes.
Gametes contain 23 chromosomes. Fertilisation restores the diploid number of 46.
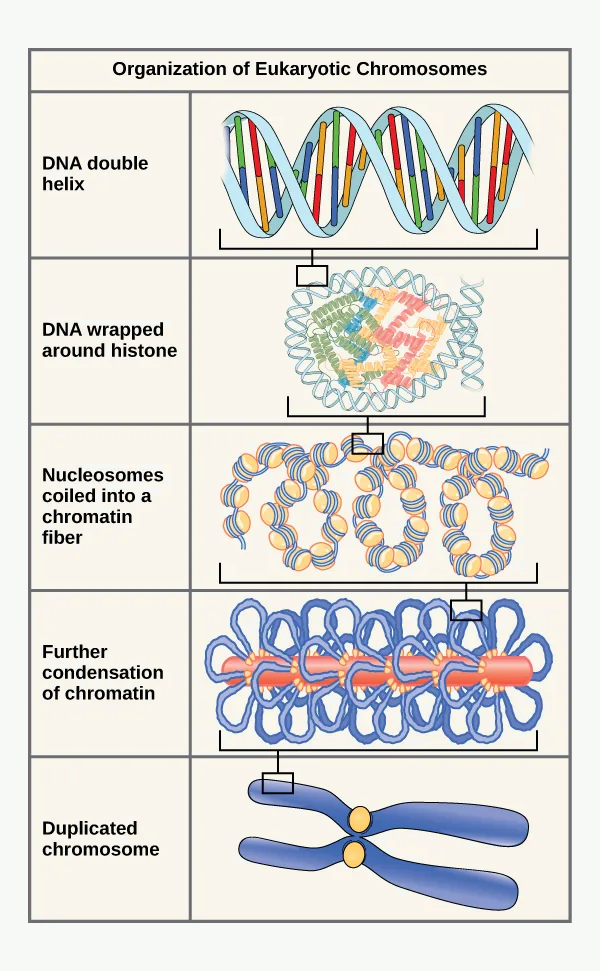
#f7f9f7; original diagram content otherwise unchanged. Source link: openstax.org/books/biology-2e/pages/14-2-dna-structure-and-sequencing.
Abbreviations shown: DNA = deoxyribonucleic acid.
How to use this figure: understand scale and packaging. A gene is a functional DNA sequence at a locus, while a chromosome is a large packaged DNA-protein structure carrying many genes.
Gene, Allele, Locus, Genotype, Phenotype
These terms are frequently confused, so they must be precise.
| Term | Meaning |
|---|---|
| Gene | A DNA sequence that encodes a functional product, usually a protein or functional RNA |
| Locus | The physical position of a gene on a chromosome |
| Allele | A version of a gene at a particular locus |
| Genotype | The genetic makeup of an individual at one or more loci |
| Phenotype | The observable trait or clinical expression resulting from genotype and environment |
Example: a patient may have a genetic variant in the pseudocholinesterase gene. The genotype is the inherited variant. The phenotype is prolonged paralysis after suxamethonium.
Genotype is not always destiny. Phenotype depends on penetrance, expressivity, environment, drugs, age, disease, and physiological stress.
Mutation and Polymorphism
A mutation is a change in DNA sequence. It may be harmful, beneficial, or neutral.
A polymorphism is a DNA sequence variation that is common in the population. Many polymorphisms have little clinical effect, but some alter drug metabolism or disease risk.
| Mutation type | Description | Possible effect |
|---|---|---|
| Silent | Codon changes but amino acid unchanged | Usually no protein change |
| Missense | One amino acid substituted for another | Mild to severe protein dysfunction |
| Nonsense | Codon becomes stop codon | Truncated protein |
| Frameshift | Insertion/deletion changes reading frame | Usually severe protein abnormality |
| Splice-site | Alters RNA splicing | Abnormal mRNA/protein |
| Duplication | Extra DNA segment | Increased or abnormal protein |
| Deletion | DNA segment lost | Loss of protein/function |
| Repeat expansion | Repeated sequence expands | Often neurological disease |
Anaesthetic relevance:
- A single amino acid substitution can change enzyme activity.
- Receptor mutations can alter drug response.
- Ion channel mutations can cause arrhythmia, myopathy, or altered muscle physiology.
- Some mutations are silent until exposed to anaesthetic triggers.
Penetrance and Expressivity
Penetrance describes whether a person with a disease-causing genotype actually shows the phenotype.
- Complete penetrance: everyone with the genotype shows the disease.
- Incomplete penetrance: some people with the genotype do not show the disease.
Expressivity describes the severity or range of features in those who express the phenotype.
Example: malignant hyperthermia susceptibility is inherited, but a patient may have several uneventful anaesthetics before developing a crisis. This reflects variable expression and the need for exposure to a trigger.
Quick check: genotype to phenotype
How do you move from DNA sequence to clinical anaesthetic risk?
Reveal answer
DNA sequence affects RNA, RNA affects protein, and protein effects determine enzyme, receptor, channel, transporter, or structural function.
Why does a mutation not automatically mean disease?
Reveal answer
The effect depends on the mutation site, protein consequence, expression, dominance, penetrance, environment, and exposure to triggers.
What do penetrance and expressivity add to clinical thinking?
Reveal answer
Penetrance asks whether the phenotype appears; expressivity asks how severe or varied it is when it appears.
EDAIC trap: central dogma questions are not about drawing DNA. They test whether you can connect DNA sequence, RNA processing, protein folding, and final anaesthetic phenotype.
DNA Replication, Transcription, and Translation
The Central Dogma
The classical flow of genetic information is:
DNA -> RNA -> Protein
This is the useful clinical chain: DNA stores the inherited instruction, RNA transfers and processes that instruction, and protein becomes the working molecule that changes drug response, enzyme activity, calcium handling, or cellular energy use.
DNA is the master recipe book in the library. mRNA is a photocopy of one recipe. The ribosome is the kitchen. The protein is the finished meal.
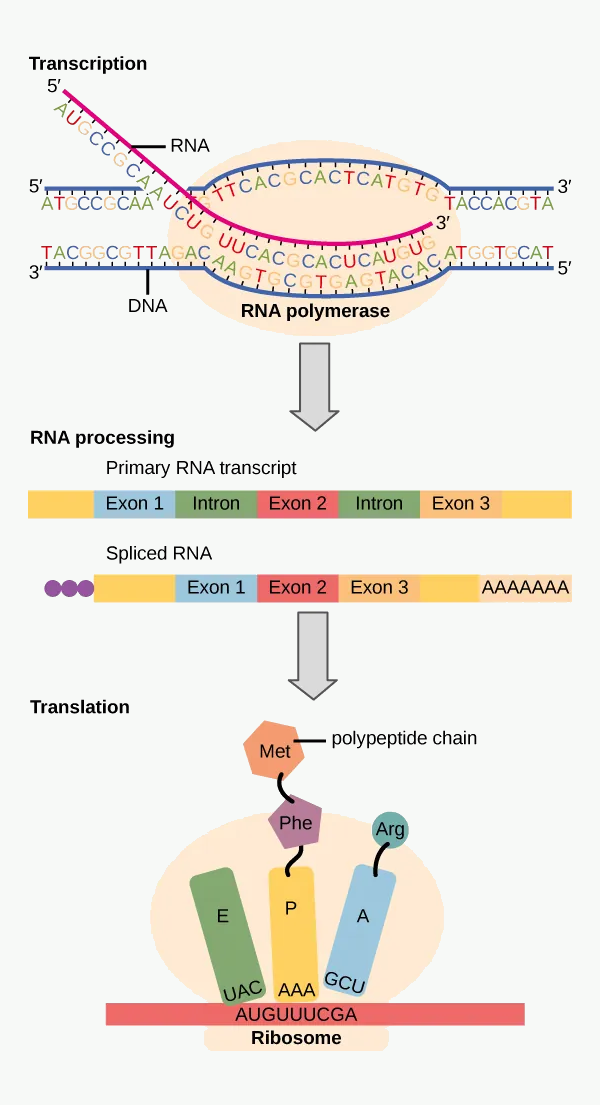
#f7f9f7; original diagram content otherwise unchanged. Source link: openstax.org/books/biology-2e/pages/15-1-the-genetic-code.
Abbreviations shown: DNA = deoxyribonucleic acid; RNA = ribonucleic acid.
How to use this figure: treat it as the module spine. DNA sequence changes can alter RNA, protein structure, enzyme activity, receptor/channel behaviour, and ultimately anaesthetic drug response.
DNA Replication
DNA replication occurs before cell division. It is semi-conservative: each new DNA molecule contains one original strand and one newly synthesised strand.
Simplified steps:
- DNA helicase unwinds the double helix.
- The two strands separate.
- DNA polymerase adds complementary nucleotides.
- One strand is copied continuously; the other is copied in fragments.
- DNA ligase joins fragments.
- Proofreading reduces errors.
Clinical relevance:
- Rapidly dividing cells are vulnerable to drugs that impair DNA replication.
- Chemotherapy, radiation, and some antimicrobials target nucleic acid synthesis.
- DNA repair defects may predispose to malignancy.
Transcription: DNA to RNA
Transcription is the production of RNA from a DNA template.
Key features:
- occurs in the nucleus,
- RNA polymerase binds to a promoter region,
- RNA is made complementary to the DNA template strand,
- RNA contains uracil instead of thymine.
| DNA | RNA equivalent |
|---|---|
| Adenine | Adenine |
| Guanine | Guanine |
| Cytosine | Cytosine |
| Thymine | Uracil replaces thymine |
RNA uses A, U, G, C.
RNA Processing
In eukaryotic cells, the first RNA transcript is called pre-mRNA. It must be processed before translation.
Processing includes:
- 5' cap - protects RNA and helps ribosome binding.
- Poly-A tail - improves stability and export from nucleus.
- Splicing - removes introns and joins exons.
| Term | Meaning |
|---|---|
| Exon | Coding sequence retained in mature mRNA |
| Intron | Non-coding sequence removed during splicing |
| Splicing | Removal of introns and joining of exons |
Alternative splicing allows one gene to produce several protein variants. This helps explain how a limited number of genes can generate many proteins.
Translation: RNA to Protein
Translation is protein synthesis from mRNA. It occurs on ribosomes in the cytoplasm or rough endoplasmic reticulum.
| Molecule | Role |
|---|---|
| mRNA | Carries codon sequence |
| Ribosome | Site of protein synthesis |
| tRNA | Brings specific amino acids |
| Amino acids | Building blocks of protein |
| rRNA | Structural/catalytic component of ribosome |
The ribosome reads mRNA in groups of three bases called codons. Each codon specifies an amino acid or stop signal.
Examples:
- AUG is the start codon and codes for methionine.
- UAA, UAG, and UGA are stop codons.
The genetic code is triplet, non-overlapping, degenerate, and nearly universal.
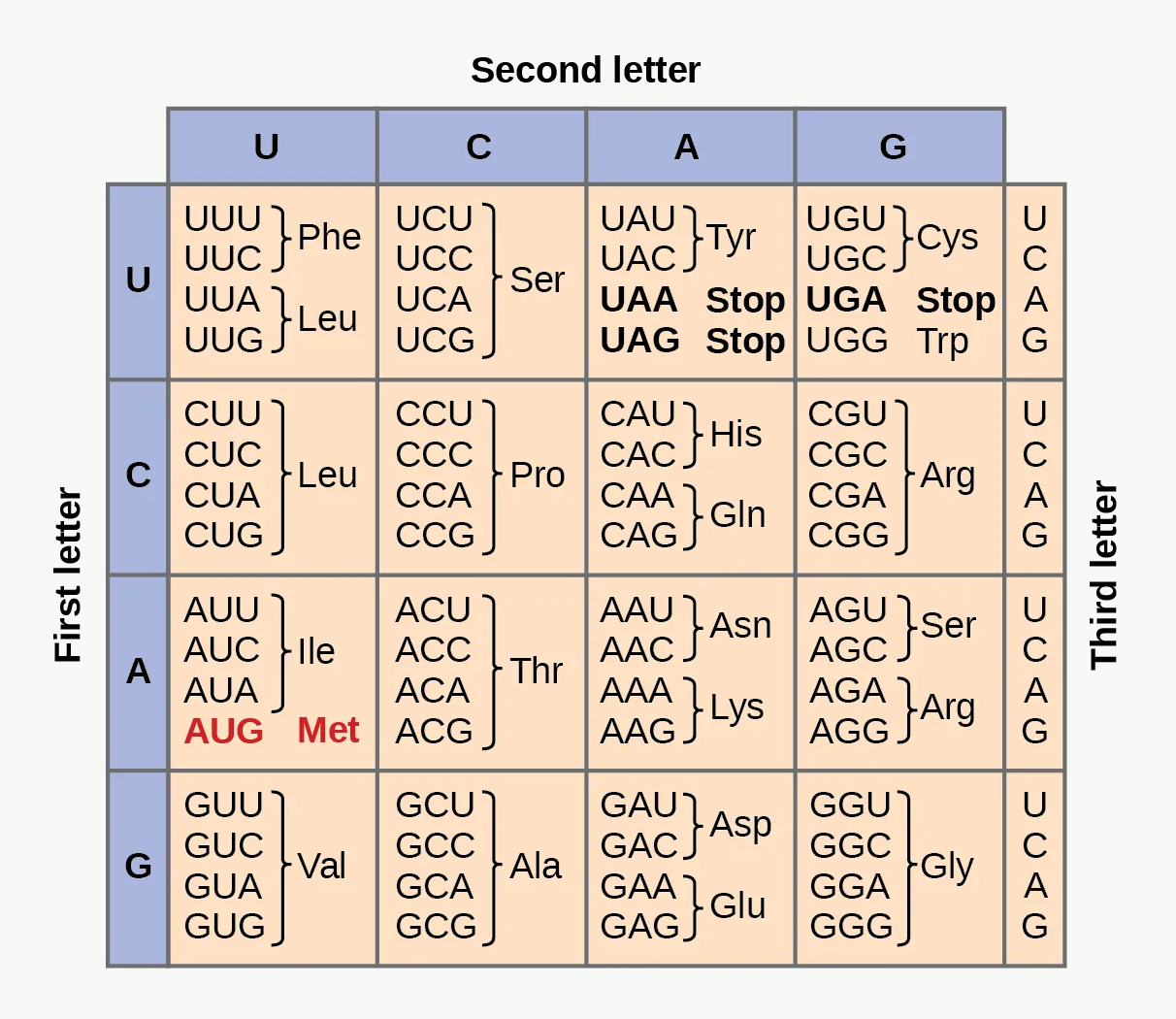
#f7f9f7; original diagram content otherwise unchanged. Source link: openstax.org/books/biology-2e/pages/15-1-the-genetic-code.
Abbreviations shown: A = adenine; U = uracil; G = guanine; C = cytosine; Phe = phenylalanine; Leu = leucine; Ser = serine; Tyr = tyrosine; Cys = cysteine; Trp = tryptophan; Pro = proline; His = histidine; Gln = glutamine; Arg = arginine; Ile = isoleucine; Met = methionine; Thr = threonine; Asn = asparagine; Lys = lysine; Val = valine; Ala = alanine; Asp = aspartate; Glu = glutamate; Gly = glycine.
How to use this figure: do not memorise the whole table. Learn that codons are triplets, AUG codes for methionine/start, stop codons terminate translation, and mutation impact depends on codon change.
From Amino Acid Chain to Functional Protein
Translation produces a chain of amino acids. The chain must fold into a specific three-dimensional shape to become a functioning protein.
| Level | Description |
|---|---|
| Primary | Amino acid sequence |
| Secondary | Alpha helices and beta sheets |
| Tertiary | Full 3D folding of one polypeptide |
| Quaternary | Assembly of multiple subunits |
Examples:
- Haemoglobin has quaternary structure.
- Ion channels are protein complexes.
- Receptors have specific binding sites.
- Enzymes need correct folding for active-site function.
A mutation that changes one amino acid can alter folding, activity, stability, receptor binding, or degradation.
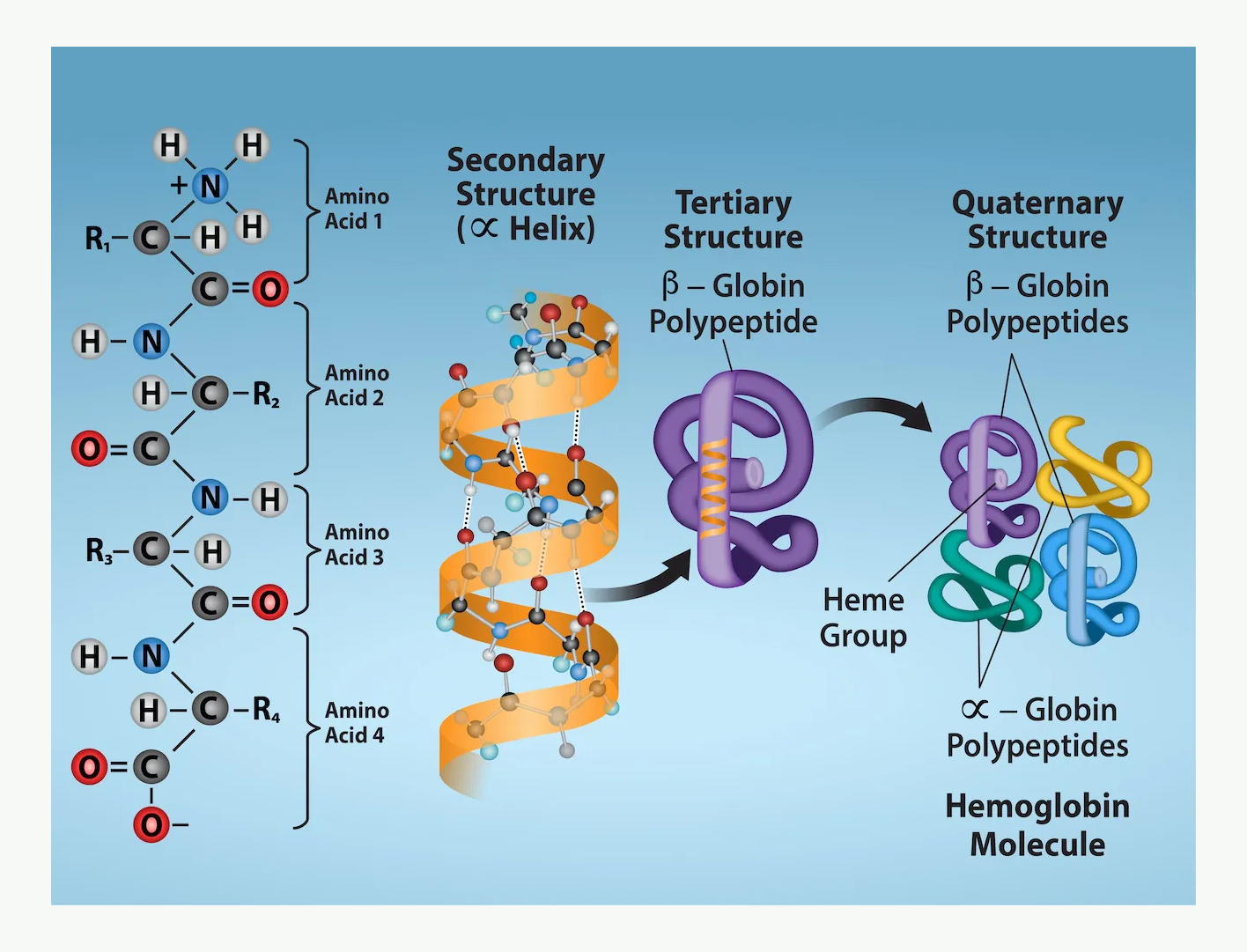
How to use this figure: connect structure to function. A single amino-acid substitution can alter folding, channel gating, receptor binding, enzyme activity, or protein stability.
Post-Translational Modification
After translation, proteins may be modified by phosphorylation, glycosylation, acetylation, methylation, hydroxylation, disulfide bond formation, cleavage of inactive precursors, or addition of lipid groups.
Clinical relevance:
- Many signalling pathways depend on phosphorylation.
- Glycoproteins are important in receptors and cell recognition.
- Clotting factors require vitamin K dependent post-translational modification.
- Insulin is produced from a precursor molecule.
- Collagen requires hydroxylation, which depends on vitamin C.
Quick check: central dogma and protein function
What is the practical meaning of DNA to RNA to protein?
Reveal answer
DNA stores sequence information, transcription produces RNA, and translation produces the amino-acid chain that folds into a functioning protein.
Why is protein folding clinically important?
Reveal answer
Folding creates the active site, receptor-binding region, channel gate, or structural shape. A small sequence change can therefore produce a large functional effect.
Which codon points are worth knowing rather than memorising the entire code?
Reveal answer
Codons are triplets; AUG is start and methionine; UAA, UAG, and UGA are stop codons.
EDAIC trap: autosomal dominant does not mean every carrier is clinically obvious. Penetrance, expressivity, and exposure to triggers explain why family history can be misleading.
Inheritance Patterns
Autosomal Dominant Inheritance
A single abnormal allele on an autosome can cause disease.
Features:
- usually affects males and females equally,
- often appears in every generation,
- an affected heterozygous parent has a 50% chance of passing the variant to each child,
- severity may vary because of penetrance and expressivity.
Anaesthetic example: malignant hyperthermia susceptibility is classically autosomal dominant.
Autosomal Recessive Inheritance
Two abnormal alleles are usually required for disease.
Features:
- parents may be asymptomatic carriers,
- males and females affected equally,
- more common with consanguinity,
- if both parents are carriers: 25% affected, 50% carriers, 25% unaffected non-carriers for each pregnancy.
Anaesthetic example: clinically significant pseudocholinesterase deficiency often behaves as an autosomal recessive condition, although heterozygotes may have intermediate enzyme activity and modestly prolonged blockade.
X-Linked Inheritance
The gene is on the X chromosome.
In X-linked recessive disease:
- males are more commonly affected,
- females may be carriers,
- affected males transmit the variant to all daughters and no sons,
- carrier females have a 50% chance of passing the variant to each child.
Some neuromuscular disorders with anaesthetic implications are X-linked. A careful family history may reveal affected male relatives.
Mitochondrial Inheritance
Mitochondria have their own DNA. Mitochondrial DNA is inherited almost entirely from the mother.
Features:
- affected mothers may pass the mutation to all children,
- affected fathers usually do not transmit mitochondrial DNA,
- organs with high energy demand are commonly affected: brain, muscle, heart, liver,
- disease severity depends on the proportion of abnormal mitochondria in tissues.
Anaesthetic relevance: patients with mitochondrial disease may be vulnerable to fasting, hypoglycaemia, hypothermia, lactate accumulation, and impaired response to metabolic stress.
Multifactorial Inheritance
Many traits and diseases result from multiple genes plus environmental factors.
Examples relevant to anaesthesia and ICU include obesity, hypertension, diabetes mellitus, coronary artery disease, many drug responses, postoperative nausea and vomiting tendency, and thrombosis risk.
The exam point is that not every inherited tendency follows simple Mendelian rules.
Quick check: inheritance patterns
What is the typical autosomal dominant risk from an affected heterozygous parent?
Reveal answer
Each child has a 50% chance of inheriting the pathogenic allele, although clinical expression can vary.
What is the classic carrier-parent risk in autosomal recessive inheritance?
Reveal answer
If both parents are carriers, each pregnancy has a 25% affected, 50% carrier, and 25% unaffected non-carrier pattern.
Why can mitochondrial disease severity be variable?
Reveal answer
Mitochondrial DNA is maternally transmitted, but tissue severity depends on the proportion of abnormal mitochondria in energy-demanding organs.
EDAIC trap: biochemistry matters when physiology fails. ATP depletion turns molecular pathways into clinical problems: pump failure, calcium overload, acidosis, rhabdomyolysis, and organ injury.
Basic Biochemistry for Anaesthetists
Why Biochemistry Matters in Anaesthesia
Biochemistry explains how cells generate energy, build proteins, metabolise drugs, respond to hypoxia, and fail during shock.
Anaesthetic examples:
- Hypoxia limits oxidative phosphorylation.
- Sepsis impairs cellular oxygen use.
- Propofol, opioids, local anaesthetics, and volatile agents act on proteins.
- Enzyme activity determines drug clearance.
- Starvation and stress can trigger acute porphyria.
- Hypermetabolism in malignant hyperthermia produces CO2, lactate, heat, and rhabdomyolysis.
Amino Acids and Proteins
Proteins are polymers of amino acids joined by peptide bonds.
Proteins function as enzymes, receptors, ion channels, transporters, structural proteins, hormones, antibodies, clotting factors, and contractile proteins.
Anaesthetic drugs mostly act on proteins, not on lipids alone.
| Drug/class | Main protein target |
|---|---|
| Local anaesthetics | Voltage-gated Na+ channels |
| Benzodiazepines | GABA-A receptor |
| Propofol | GABA-A receptor and other CNS targets |
| Opioids | mu, kappa, delta opioid receptors |
| Non-depolarising muscle relaxants | Nicotinic acetylcholine receptor |
| Suxamethonium | Nicotinic acetylcholine receptor |
| Dantrolene | Ryanodine receptor |
| Neostigmine | Acetylcholinesterase |
Denaturation and Protein Dysfunction
Protein shape determines function. Denaturation means loss of normal three-dimensional structure.
Causes include extreme temperature, severe pH disturbance, chemical injury, oxidative stress, heavy metals, and severe inflammation.
Clinical relevance:
- Hyperthermia can impair enzyme function.
- Acidosis reduces myocardial performance and alters drug binding.
- Alkalosis changes ionised calcium and neuromuscular excitability.
- Sepsis and reperfusion injury produce oxidative stress.
Carbohydrates and Glucose Metabolism
Glucose is a major cellular fuel, especially for the brain, red blood cells, renal medulla, and exercising muscle.
| Pathway | Main role |
|---|---|
| Glycolysis | Glucose to pyruvate; produces small amount of ATP |
| Glycogenesis | Storage of glucose as glycogen |
| Glycogenolysis | Breakdown of glycogen to glucose |
| Gluconeogenesis | New glucose production from lactate, glycerol, amino acids |
| Pentose phosphate pathway | NADPH production and ribose synthesis |
Red blood cells have no mitochondria, so they depend entirely on glycolysis.
Aerobic and Anaerobic Metabolism
Under aerobic conditions:
Glucose -> pyruvate -> acetyl-CoA -> citric acid cycle -> oxidative phosphorylation -> ATP
This produces much more ATP than anaerobic metabolism.
Under anaerobic conditions:
Pyruvate -> lactate
This regenerates NAD+ so glycolysis can continue, but ATP yield is low.
Clinical relevance:
- In shock, oxygen delivery may be inadequate; lactate rises.
- Lactate may also rise from beta-agonists, seizures, hepatic failure, mitochondrial dysfunction, and regional ischaemia.
- A raised lactate is not always pure hypoxia, but in anaesthesia and ICU it is always a warning sign that tissue metabolism or clearance is abnormal.
ATP: The Cellular Currency
ATP powers ion pumps such as Na+/K+-ATPase, Ca2+ reuptake into sarcoplasmic reticulum, muscle contraction and relaxation, vesicle transport, biosynthesis, active transport, and cell repair mechanisms.
When ATP fails:
- Na+/K+-ATPase fails,
- intracellular Na+ rises,
- water enters cells,
- cells swell,
- Ca2+ accumulates,
- enzymes activate abnormally,
- mitochondrial injury worsens,
- apoptosis or necrosis may follow.
This is why hypoxia and ischaemia cause cellular swelling and organ dysfunction.
Lipids
Lipids include triglycerides, phospholipids, cholesterol, and steroid molecules.
Functions include energy storage, membrane structure, steroid hormone synthesis, signalling molecules, insulation, and drug distribution compartments.
Anaesthetic relevance:
- Lipid-soluble drugs cross membranes and the blood-brain barrier more readily.
- Highly lipid-soluble drugs may redistribute into fat.
- Local anaesthetic systemic toxicity is treated with lipid emulsion therapy.
- Steroid synthesis depends on cholesterol.
- Propofol is formulated in lipid emulsion.
Heme Synthesis as a Bridge to Porphyria
Heme is required for haemoglobin, myoglobin, cytochromes, catalase, peroxidases, and nitric oxide synthase.
Heme synthesis occurs partly in mitochondria and partly in cytosol. The first and rate-limiting step in hepatic heme synthesis is catalysed by ALA synthase 1.
Why anaesthetists care: drugs that induce hepatic cytochrome P450 increase heme demand. If the patient has an inherited enzyme defect in the heme pathway, increased pathway flux can lead to accumulation of toxic precursors and an acute porphyric crisis.

#f7f9f7 with no alteration to pathway text, arrows, or diagram structure. Source link: commons.wikimedia.org/wiki/File:Heme_synthesis.svg.
Abbreviations shown: Fe2+ = ferrous iron; mRNA = messenger ribonucleic acid; ALA = aminolevulinic acid; PB = porphobilinogen; UP III = uroporphyrinogen III; CP-III = coproporphyrinogen III; CO2 = carbon dioxide.
How to use this figure: focus on pathway induction and precursor accumulation. Acute porphyrias become dangerous when drugs, fasting, or stress increase hepatic ALA synthase activity in a vulnerable pathway.
Quick check: proteins, ATP, enzymes and haem
Why do anaesthetic drugs mostly act through proteins?
Reveal answer
Their key targets are receptors, ion channels, enzymes, transporters, and contractile proteins, all of which depend on protein structure and function.
What happens when ATP supply fails during hypoxia or ischaemia?
Reveal answer
Ion pumps fail, sodium and calcium accumulate intracellularly, water enters cells, mitochondria worsen, and cell injury progresses.
Why does haem synthesis link biochemistry to anaesthetic risk?
Reveal answer
Drugs, fasting, and stress can increase hepatic haem pathway flux; in acute porphyria this can accumulate neurotoxic precursors.
EDAIC trap: pharmacogenetics is not only drug metabolism. Genetic variation may change pharmacokinetics, but it may also change receptors, ion channels, enzyme targets, and crisis susceptibility.
Pharmacogenetics and Anaesthetic Drug Response
What Is Pharmacogenetics?
Pharmacogenetics is the study of how inherited genetic variation affects drug response.
Drug response depends on absorption, distribution, metabolism, excretion, receptor structure, channel function, enzyme activity, transporters, disease state, age, organ function, and concurrent drugs.
Genetics is only one part, but sometimes it is decisive.
Pharmacokinetic Variation
Pharmacokinetics asks: what does the body do to the drug?
Genetic variation may affect hepatic enzymes, plasma enzymes, renal transporters, plasma protein levels, and active transporters such as P-glycoprotein.
Examples:
- Pseudocholinesterase variants prolong suxamethonium and mivacurium effect.
- CYP2D6 variation affects codeine and tramadol activation.
- CYP2C19 variation affects some proton pump inhibitors and clopidogrel.
- CYP2C9/VKORC1 variation affects warfarin sensitivity.
Pharmacodynamic Variation
Pharmacodynamics asks: what does the drug do to the body?
Genetic variation may affect receptor sensitivity, ion channel behaviour, intracellular signalling, muscle calcium release, and enzyme target sensitivity.
Examples:
- RYR1 mutation predisposes to malignant hyperthermia.
- Cardiac ion channel mutations may predispose to arrhythmia under stress or with QT-prolonging drugs.
- Receptor variation may influence opioid or beta-agonist response.
EDAIC trap: acute porphyria is mainly a neurovisceral crisis, not simply abdominal pain and not primarily a skin disease. Drug safety must be checked with current porphyria guidance.
Porphyria
Definition
Porphyrias are inherited or acquired disorders of heme biosynthesis. The anaesthetic concern is mainly the acute hepatic porphyrias, especially acute intermittent porphyria.
Acute porphyria is a disorder of heme synthesis in which stressors such as unsafe drugs, fasting, dehydration, infection, alcohol, or hormones can increase hepatic heme pathway activity and cause accumulation of neurotoxic precursors.
Heme Pathway Mechanism
Heme synthesis requires several enzymes. If one enzyme is deficient, pathway intermediates accumulate.
In acute hepatic porphyrias, the important toxic precursors are ALA and PBG. These are associated with neurological and autonomic symptoms.
The hepatic rate-limiting enzyme is ALA synthase 1. It is upregulated when hepatic heme demand rises, especially when cytochrome P450 enzymes are induced.
Triggers of Acute Attack
Common triggers include unsafe drugs, fasting or low carbohydrate intake, dehydration, infection, alcohol, stress, surgery, hormonal changes, smoking, and severe illness.
Anaesthesia combines several triggers: fasting, surgical stress, drug exposure, pain, nausea, dehydration, and infection risk. Safe perioperative planning is therefore essential.
Clinical Features of Acute Porphyria
Think of acute porphyria as a neurovisceral crisis.
| System | Features |
|---|---|
| Gastrointestinal | Severe abdominal pain, nausea, vomiting, constipation |
| Autonomic | Tachycardia, hypertension, sweating, fever |
| Neurological | Peripheral neuropathy, weakness, seizures, respiratory failure |
| Psychiatric | Anxiety, agitation, hallucinations, confusion |
| Electrolytes | Hyponatraemia, often from SIADH or vomiting/dehydration |
| Urine | Dark or reddish urine may occur |
Important exam point:
- Acute intermittent porphyria usually does not cause photosensitive skin lesions.
- Cutaneous porphyrias cause photosensitivity, but are less commonly the major anaesthetic emergency.
Anaesthetic Management Principles in Porphyria
The safest approach is not to memorise one fixed drug list forever. Drug safety classifications can change and vary between databases.
For any patient with acute porphyria, check an up-to-date porphyria drug safety database and avoid porphyrinogenic drugs.
General principles:
- Avoid prolonged fasting.
- Avoid dehydration.
- Give carbohydrate-containing fluid if oral intake is delayed.
- Treat pain, nausea, and infection aggressively using safe drugs.
- Avoid known unsafe or uncertain drugs.
- Minimise surgical stress.
- Monitor sodium, neurological status, and autonomic signs.
- In an acute attack, seek specialist advice and consider hemin or haem arginate where available.
Classic drugs to avoid or treat with caution in exams include barbiturates, especially thiopental; etomidate; many enzyme-inducing anticonvulsants; some sulphonamides; rifampicin; alcohol; and other drugs listed as unsafe in current porphyria databases.
Commonly used anaesthetic options generally considered acceptable in many modern references include propofol, opioids, benzodiazepines, non-depolarising neuromuscular blockers, nitrous oxide, many volatile agents, and local anaesthetics depending on database classification. The exam-safe wording is: check the current porphyria-safe drug list.
Exam Traps in Porphyria
- Porphyria is not one disease; acute hepatic porphyrias are the main anaesthetic concern.
- Fasting is a trigger; avoid unnecessary starvation.
- Barbiturates are classic unsafe drugs.
- Abdominal pain with normal abdominal findings, tachycardia, hypertension, neuropsychiatric signs, and hyponatraemia should suggest acute porphyria.
- Treating pain and nausea matters because stress and poor intake worsen attacks.
- Always check drug safety rather than relying on memory alone.
Quick check: pharmacogenetics and porphyria
How can pharmacogenetics change drug response?
Reveal answer
Inherited variation can alter metabolism, transport, receptor sensitivity, channel behaviour, or enzyme target response.
What pattern should make acute porphyria enter the differential?
Reveal answer
Severe abdominal pain with autonomic signs, neuropsychiatric features, weakness or seizures, hyponatraemia, and a trigger such as fasting or unsafe drugs.
What is the exam-safe drug principle in acute porphyria?
Reveal answer
Use an up-to-date porphyria drug safety database, avoid porphyrinogenic drugs, prevent fasting, and treat pain, nausea, dehydration, and infection.
EDAIC trap: fever may be late in malignant hyperthermia. Rising end-tidal CO2, tachycardia, rigidity, acidosis, and hyperkalaemia are earlier danger signals.
Malignant Hyperthermia
Definition
Malignant hyperthermia is an inherited skeletal muscle disorder causing a hypermetabolic crisis after exposure to triggering anaesthetic agents.
Malignant hyperthermia is an inherited disorder of skeletal muscle calcium regulation, usually involving the ryanodine receptor, triggered mainly by volatile anaesthetics and suxamethonium, causing uncontrolled calcium release, muscle rigidity, hypermetabolism, acidosis, hyperkalaemia, rhabdomyolysis, and heat production.
Genetics
Malignant hyperthermia susceptibility is classically autosomal dominant with variable penetrance.
Important genes:
- RYR1: ryanodine receptor type 1 in skeletal muscle; the most important.
- CACNA1S: dihydropyridine receptor/L-type calcium channel subunit; less common.
A patient may have had previous uneventful anaesthetics and still be susceptible.
Normal Skeletal Muscle Calcium Handling
Normal excitation-contraction coupling:
- Motor nerve releases acetylcholine at the neuromuscular junction.
- Muscle membrane depolarises.
- Depolarisation travels down T-tubules.
- Dihydropyridine receptors sense depolarisation.
- Ryanodine receptors open on sarcoplasmic reticulum.
- Calcium is released into cytosol.
- Calcium binds troponin C.
- Actin-myosin cross-bridge cycling causes contraction.
- Calcium is pumped back into sarcoplasmic reticulum by Ca2+-ATPase.
- Muscle relaxes.
What Goes Wrong in Malignant Hyperthermia?
In susceptible skeletal muscle, triggering agents cause abnormal ryanodine receptor opening and uncontrolled calcium release from the sarcoplasmic reticulum.
| Triggered calcium release causes | Clinical consequence |
|---|---|
| Sustained contraction | Rigidity, masseter spasm |
| Massive ATP consumption | Heat generation and metabolic stress |
| Increased oxygen consumption | Desaturation risk and cyanosis if severe |
| Increased CO2 production | Rising end-tidal CO2, respiratory acidosis |
| Anaerobic metabolism | Lactic acidosis |
| Muscle breakdown | Rhabdomyolysis, myoglobinuria, acute kidney injury |
| Potassium release | Hyperkalaemia and arrhythmias |
The earliest sign is often unexpected rise in end-tidal CO2, not fever. Fever may be late.
Triggers and Safe Agents
Classic triggers:
- all potent volatile anaesthetic agents,
- suxamethonium.
Non-triggers include propofol, opioids, benzodiazepines, ketamine, etomidate, nitrous oxide, local anaesthetics, non-depolarising neuromuscular blockers, and reversal agents.
For a susceptible patient, use a trigger-free anaesthetic, commonly total intravenous anaesthesia, regional anaesthesia where appropriate, and a prepared anaesthetic machine free from volatile contamination.
Clinical Features
Early signs:
- unexpected rise in end-tidal CO2,
- tachycardia,
- tachypnoea if spontaneously breathing,
- increased oxygen consumption,
- masseter spasm after suxamethonium,
- generalised muscle rigidity,
- mixed respiratory and metabolic acidosis.
Later signs:
- hyperthermia,
- hyperkalaemia,
- arrhythmias,
- myoglobinuria,
- raised creatine kinase,
- disseminated intravascular coagulation,
- acute kidney injury.
The name malignant hyperthermia is slightly misleading because temperature rise is not always the first sign.
Management of Malignant Hyperthermia Crisis
Immediate actions:
- Call for help.
- Stop volatile agents and suxamethonium.
- Maintain anaesthesia with non-triggering agents.
- Hyperventilate with 100% oxygen using high fresh gas flow.
- Give dantrolene immediately.
- Actively cool if hyperthermic.
- Treat hyperkalaemia.
- Treat acidosis.
- Treat arrhythmias, avoiding calcium channel blockers with dantrolene.
- Maintain urine output and manage rhabdomyolysis.
- Send blood gases, electrolytes, CK, coagulation, renal function, and urine myoglobin if available.
- Transfer to ICU for monitoring because recrudescence can occur.
Dantrolene initial dose is commonly 2.5 mg/kg IV, repeated until signs improve. Ongoing dosing or infusion may be needed.
Mechanism: dantrolene acts on skeletal muscle ryanodine receptor-mediated calcium release, reducing further calcium release from the sarcoplasmic reticulum.
Management of Known or Suspected MH Susceptibility
Preoperative plan:
- take family history seriously,
- avoid volatile agents and suxamethonium,
- use regional anaesthesia if suitable,
- use TIVA if general anaesthesia required,
- prepare anaesthetic machine according to local MH protocol,
- ensure dantrolene availability,
- use standard monitoring including capnography and temperature,
- document clearly,
- refer for specialist MH investigation when appropriate.
Important point: a normal previous anaesthetic does not exclude MH susceptibility.
Exam Traps in Malignant Hyperthermia
- Hypercapnia is usually earlier than hyperthermia.
- The basic defect is skeletal muscle calcium handling.
- The key receptor is RYR1, the skeletal muscle ryanodine receptor.
- Volatile agents and suxamethonium are triggers.
- Nitrous oxide, propofol, opioids, local anaesthetics, and non-depolarising relaxants are safe for MH.
- Dantrolene is specific treatment.
- Masseter spasm after suxamethonium may be an early warning sign.
- Treat hyperkalaemia and rhabdomyolysis aggressively.
EDAIC trap: pseudocholinesterase deficiency prolongs drug exposure; it does not mean the nicotinic receptor is abnormal. The immediate management is sedation, ventilation, and time.
Pseudocholinesterase Deficiency
Definition
Pseudocholinesterase deficiency is a genetic or acquired reduction in plasma cholinesterase activity, causing prolonged action of drugs normally metabolised by this enzyme, especially suxamethonium and mivacurium.
Pseudocholinesterase deficiency is reduced or abnormal plasma butyrylcholinesterase activity, leading to prolonged neuromuscular blockade after suxamethonium or mivacurium.
The Enzyme
Pseudocholinesterase is also called plasma cholinesterase or butyrylcholinesterase. It is produced mainly in the liver and found in plasma.
It metabolises suxamethonium, mivacurium, ester local anaesthetics to varying degrees, and cocaine.
It is different from acetylcholinesterase, which is found at cholinergic synapses and the neuromuscular junction.

#f7f9f7; neuromuscular junction structures, labels, and lines otherwise unchanged. Source link: commons.wikimedia.org/wiki/File:Neuromuscular_junction.svg.
Abbreviations shown: ACh = acetylcholine.
How to use this figure: locate where suxamethonium acts and why prolonged plasma persistence matters. Pseudocholinesterase deficiency does not change the receptor; it prolongs exposure to a depolarising blocker.
Normal Suxamethonium Metabolism
Suxamethonium is a depolarising neuromuscular blocker. Normally, it is rapidly hydrolysed by plasma cholinesterase before much of it reaches the neuromuscular junction. This gives it a short duration of action.
If pseudocholinesterase activity is reduced or abnormal:
- suxamethonium is metabolised slowly,
- the depolarising block is prolonged,
- the patient remains paralysed and apnoeic,
- consciousness may return before muscle power unless sedation is maintained.
This is a patient safety emergency because awareness with paralysis is possible if not recognised.
Genetics
Clinically important inherited pseudocholinesterase deficiency is commonly autosomal recessive.
Variants include usual/normal allele, atypical dibucaine-resistant allele, fluoride-resistant allele, and silent allele with little or no enzyme activity.
Heterozygotes may have modest prolongation. Homozygotes for abnormal variants may have very prolonged paralysis.
Dibucaine Number
Dibucaine inhibits normal pseudocholinesterase more than atypical enzyme. The dibucaine number is the percentage inhibition of enzyme activity by dibucaine.
Dibucaine number reflects enzyme quality, not enzyme quantity.
| Phenotype | Dibucaine number | Expected effect |
|---|---|---|
| Normal | ~80 | Normal suxamethonium duration |
| Heterozygous atypical | ~40-70 | Mild/moderate prolongation |
| Homozygous atypical | <30 | Marked prolongation |
Enzyme activity level measures quantity. Dibucaine number measures how abnormal the enzyme is.
Acquired Causes of Reduced Pseudocholinesterase Activity
Pseudocholinesterase activity may be reduced by pregnancy, liver disease, severe renal disease, malnutrition, malignancy, burns, severe systemic illness, organophosphate poisoning, some drugs, and cardiopulmonary bypass.
The normal reduction in pregnancy is usually not enough to cause major clinical prolongation by itself, but it can contribute in susceptible patients.
Clinical Presentation
Typical scenario: a patient receives suxamethonium for rapid sequence induction. Surgery ends. The volatile or IV anaesthetic wears off. The patient remains apnoeic with no adequate neuromuscular recovery.
Findings:
- absent or weak respiratory effort,
- low train-of-four response,
- prolonged paralysis,
- normal pupils and haemodynamics may mislead,
- consciousness may return if sedation is not maintained.
Differential diagnosis includes residual non-depolarising neuromuscular blocker, hypothermia, electrolyte disturbance, opioid or sedative overdose, central neurological cause, severe metabolic disturbance, and equipment or monitoring error.
Management
Management is supportive:
- Continue ventilation.
- Maintain sedation and amnesia.
- Monitor neuromuscular function.
- Check temperature, electrolytes, acid-base status, and drug history.
- Avoid further suxamethonium or mivacurium.
- Wait for spontaneous recovery.
- Explain to the patient after recovery.
- Document clearly.
- Arrange confirmatory testing and family screening where appropriate.
- Provide written warning for future anaesthetics.
Anticholinesterases such as neostigmine do not reliably reverse suxamethonium apnoea and may worsen depolarising block in some circumstances. Fresh frozen plasma contains enzyme and has historically been discussed, but because supportive ventilation is safe and transfusion has risks, FFP is not routine management.
Future Anaesthesia
Avoid suxamethonium and mivacurium.
Use alternatives such as rocuronium with sugammadex where appropriate, non-depolarising neuromuscular blockers with quantitative monitoring, or regional anaesthesia if suitable.
Pseudocholinesterase deficiency is not an allergy. It is an enzyme metabolism problem.
Exam Traps in Pseudocholinesterase Deficiency
- Pseudocholinesterase is plasma butyrylcholinesterase, not acetylcholinesterase at the NMJ.
- Dibucaine number measures enzyme abnormality, not enzyme concentration.
- Suxamethonium and mivacurium are the key anaesthetic drugs affected.
- Management is ventilation plus sedation until recovery.
- Neostigmine is not the solution.
- Pregnancy reduces enzyme activity, but usually not enough alone to cause severe apnoea.
- The patient must be warned and the event documented.
Quick check: inherited anaesthetic emergencies
How do you separate malignant hyperthermia from pseudocholinesterase deficiency?
Reveal answer
Malignant hyperthermia is a hypermetabolic skeletal muscle calcium-release crisis; pseudocholinesterase deficiency is prolonged neuromuscular block from slow drug metabolism.
What is the earliest classic warning sign in malignant hyperthermia?
Reveal answer
Unexpected rising end-tidal carbon dioxide is often earlier than fever, especially during controlled ventilation.
What protects the pseudocholinesterase-deficient patient after prolonged apnoea is recognised?
Reveal answer
Continue ventilation, maintain sedation and amnesia, monitor neuromuscular recovery, avoid further suxamethonium or mivacurium, and document the event clearly.
Bringing the Module Together
This module connects molecular biology to the operating theatre.
DNA contains the code. Genes are transcribed into RNA. RNA is translated into proteins. Proteins become enzymes, receptors, channels, transporters, contractile molecules, and structural components. Anaesthetic drugs interact with those proteins, and inherited variation can make that interaction unpredictable.
Three conditions show why this matters:
- Porphyria: a heme synthesis disorder where unsafe drugs, fasting, and stress can trigger neurovisceral crisis.
- Malignant hyperthermia: a skeletal muscle calcium-release disorder where volatile agents and suxamethonium can trigger a fatal hypermetabolic crisis.
- Pseudocholinesterase deficiency: a plasma enzyme abnormality where suxamethonium or mivacurium can cause prolonged paralysis.
The question is not only “what drug did I give?” but also “what biochemical system did I challenge?”
How to use these tables: read each row from mechanism to consequence to management. That sequence mirrors how EDAIC statements are usually tested.
High-Yield Tables
DNA, RNA, and Protein Synthesis
| Step | Location | Main process | Product |
|---|---|---|---|
| Replication | Nucleus | DNA copied before cell division | DNA |
| Transcription | Nucleus | DNA copied into RNA | pre-mRNA |
| RNA processing | Nucleus | Splicing, cap, poly-A tail | mature mRNA |
| Translation | Ribosome | mRNA read as codons | polypeptide |
| Post-translational modification | ER/Golgi/cytosol | Folding, cleavage, chemical modification | functional protein |
Inheritance Patterns
| Pattern | Key feature | Anaesthetic relevance |
|---|---|---|
| Autosomal dominant | One abnormal allele may cause disease | Malignant hyperthermia susceptibility |
| Autosomal recessive | Two abnormal alleles usually required | Severe pseudocholinesterase deficiency |
| X-linked recessive | Males usually more affected | Some neuromuscular diseases |
| Mitochondrial | Maternal inheritance | Mitochondrial myopathies, metabolic vulnerability |
| Multifactorial | Many genes plus environment | Common disease and variable drug response |
Three Inherited Anaesthetic Hazards
| Condition | Basic defect | Trigger/problem | Key management |
|---|---|---|---|
| Porphyria | Heme synthesis enzyme defect | Unsafe drugs, fasting, stress | Avoid triggers, safe drugs, glucose, specialist treatment |
| Malignant hyperthermia | Skeletal muscle calcium release disorder | Volatile agents, suxamethonium | Stop triggers, 100% O2, dantrolene, cooling, ICU |
| Pseudocholinesterase deficiency | Reduced/abnormal plasma cholinesterase | Suxamethonium, mivacurium | Ventilate and sedate until recovery |
Definitions and Values to Memorise
These are the terms and values most likely to appear as near-true statements. Learn them as paired distinctions, because EDAIC questions often test the boundary between similar words.
| Item | Precise recall point | Exam use |
|---|---|---|
| Human somatic chromosome number | 46 chromosomes: 22 pairs of autosomes plus one pair of sex chromosomes | Separate autosomal inheritance from sex-linked inheritance |
| DNA bases | Adenine, thymine, guanine, cytosine | RNA uses uracil instead of thymine |
| Base pairing | A-T and G-C in DNA; A-U and G-C in RNA | G-C pairing has three hydrogen bonds and is more stable than A-T |
| Codon | Three mRNA bases specifying an amino acid or a stop signal | AUG is the usual start codon and codes for methionine |
| Gene, allele, locus | Gene is a functional DNA sequence; allele is a variant; locus is physical position | Avoid using these terms interchangeably |
| Genotype versus phenotype | Genotype is inherited genetic makeup; phenotype is clinical expression | Phenotype depends on penetrance, expressivity, environment, disease, and drug exposure |
| Penetrance versus expressivity | Penetrance asks whether disease appears; expressivity asks how severe or varied it is | Explains variable malignant hyperthermia histories within families |
| Malignant hyperthermia | Autosomal dominant susceptibility, commonly RYR1; triggered by volatile agents and suxamethonium | Earliest sign is often rising end-tidal CO2, not fever |
| Dantrolene | Reduces skeletal muscle calcium release through the ryanodine receptor pathway | Specific therapy for malignant hyperthermia; not merely an antipyretic |
| Acute hepatic porphyria | Heme pathway disorder with accumulation of neurotoxic precursors such as ALA and PBG | Triggered by unsafe drugs, fasting, dehydration, infection, alcohol, surgery, hormones, and stress |
| Pseudocholinesterase deficiency | Reduced or abnormal plasma butyrylcholinesterase, causing prolonged suxamethonium or mivacurium block | Dibucaine number measures enzyme quality, not enzyme amount |
| ATP failure | Loss of ion pump function, intracellular sodium and water gain, calcium accumulation, and cell injury | Connects hypoxia, shock, mitochondrial dysfunction, and malignant hyperthermia physiology |
EDAIC Traps
Use this section as a final check before leaving the module. Each point is phrased around a common way the topic is made difficult in exam statements.
- Gene is not the same as allele. A gene is the functional DNA sequence; an allele is one version of that gene.
- Genotype is not the same as phenotype. A genotype may be silent until a drug trigger, physiological stress, or environmental exposure reveals it.
- Penetrance is not severity. Penetrance is whether the phenotype is expressed; expressivity is how it is expressed.
- RNA does not contain thymine. RNA contains uracil, and mRNA codons are read in triplets.
- Introns are removed, exons are retained. Alternative splicing can generate different proteins from one gene.
- Most mutations are not automatically clinically obvious. Silent mutations, conservative substitutions, noncoding variants, and incomplete penetrance may produce no visible phenotype.
- Mitochondrial inheritance is maternal. It does not follow classic Mendelian autosomal dominant or autosomal recessive ratios.
- Malignant hyperthermia fever can be late. Unexpected rise in end-tidal CO2, tachycardia, rigidity, acidosis, and hyperkalaemia may appear earlier.
- Dantrolene treats the calcium-release mechanism. It is not a general cooling drug and should not be delayed while waiting for hyperthermia.
- Nitrous oxide, local anaesthetics, non-depolarising neuromuscular blockers, opioids, propofol, and benzodiazepines are not classic malignant hyperthermia triggers.
- Acute intermittent porphyria is mainly neurovisceral. Photosensitivity points more toward cutaneous porphyrias.
- Dibucaine number is qualitative. Enzyme activity level is quantitative; both may be needed to interpret pseudocholinesterase results.
- Neostigmine does not rapidly reverse suxamethonium apnoea from pseudocholinesterase deficiency. Management is ventilation, sedation, monitoring, and time.
End-of-Module Summary
DNA stores genetic information. Genes are transcribed into RNA, and RNA is translated into proteins. Proteins are the practical machinery of physiology: enzymes, channels, receptors, transporters, structural molecules, clotting factors, and contractile proteins.
Inheritance may be autosomal dominant, autosomal recessive, X-linked, mitochondrial, or multifactorial. Genotype does not always predict phenotype perfectly because penetrance, expressivity, environment, drugs, and physiological stress all matter.
Biochemistry explains how cells generate ATP, use oxygen, produce lactate, synthesise heme, metabolise drugs, and fail during hypoxia or hypermetabolism.
Three inherited disorders are especially important for anaesthetists:
- Porphyria: avoid unsafe drugs, fasting, dehydration, and stress; check current drug safety guidance.
- Malignant hyperthermia: avoid volatile agents and suxamethonium in susceptible patients; treat crisis with trigger cessation, 100% oxygen, dantrolene, cooling, correction of acidosis and hyperkalaemia, and ICU care.
- Pseudocholinesterase deficiency: suspect after prolonged paralysis following suxamethonium or mivacurium; manage with ventilation, sedation, neuromuscular monitoring, documentation, and future avoidance.
Genetics explains vulnerability. Biochemistry explains mechanism. Anaesthesia reveals both.