Lecture note
Upper and Lower Airways: Structure-Function
Exam Target
Purpose. Module 1.3 connects airway anatomy to the physiological problems that anaesthetists meet immediately: obstruction, laryngospasm, aspiration, tube resistance, dry-gas injury, atelectasis, secretion retention, and surfactant failure.
Core idea. Airway structure determines airway function. Support, radius, epithelial lining, reflexes, humidification, and surface tension decide whether gas reaches the alveoli safely and whether alveoli remain open for diffusion.
Upper versus lower airway, conducting versus respiratory zone, laryngeal nerve supply, airway generations, anatomical dead space, water vapour pressure, and surfactant composition.
Why the pharynx collapses, why radius dominates resistance, why intubation changes humidification and PEEP, why cilia fail, and why surfactant stabilises small alveoli.
Airway manoeuvres, CPAP, tube size, paediatric obstruction, laryngospasm, aspiration, humidification strategy, atelectasis prevention, and neonatal or ARDS surfactant dysfunction.
Revision rule. Do not learn airway anatomy as labels only. For each structure, ask what fails under anaesthesia and which manoeuvre, device, drug, or ventilator setting compensates for that failure.
Quick check: airway structure-function frame
What is the most useful way to learn airway anatomy for anaesthesia?
Reveal answer
Attach each structure to the failure it prevents or causes: obstruction, aspiration, humidification loss, tube resistance, secretion retention, atelectasis, or surfactant failure.
What does the upper airway mainly do before gas reaches the trachea?
Reveal answer
It conducts, warms, humidifies, filters, smells, protects against aspiration, and helps coordinate speech and swallowing.
What is the distal airway goal?
Reveal answer
Deliver gas to a thin, stable, dry alveolar-capillary surface where oxygen and carbon dioxide can diffuse efficiently.
EDAIC trap: airway anatomy is rarely tested as naming alone. First identify the structure, then ask what happens when tone, radius, lining, humidity, reflexes, or surface tension fails under anaesthesia.
Overview of the Respiratory Tract
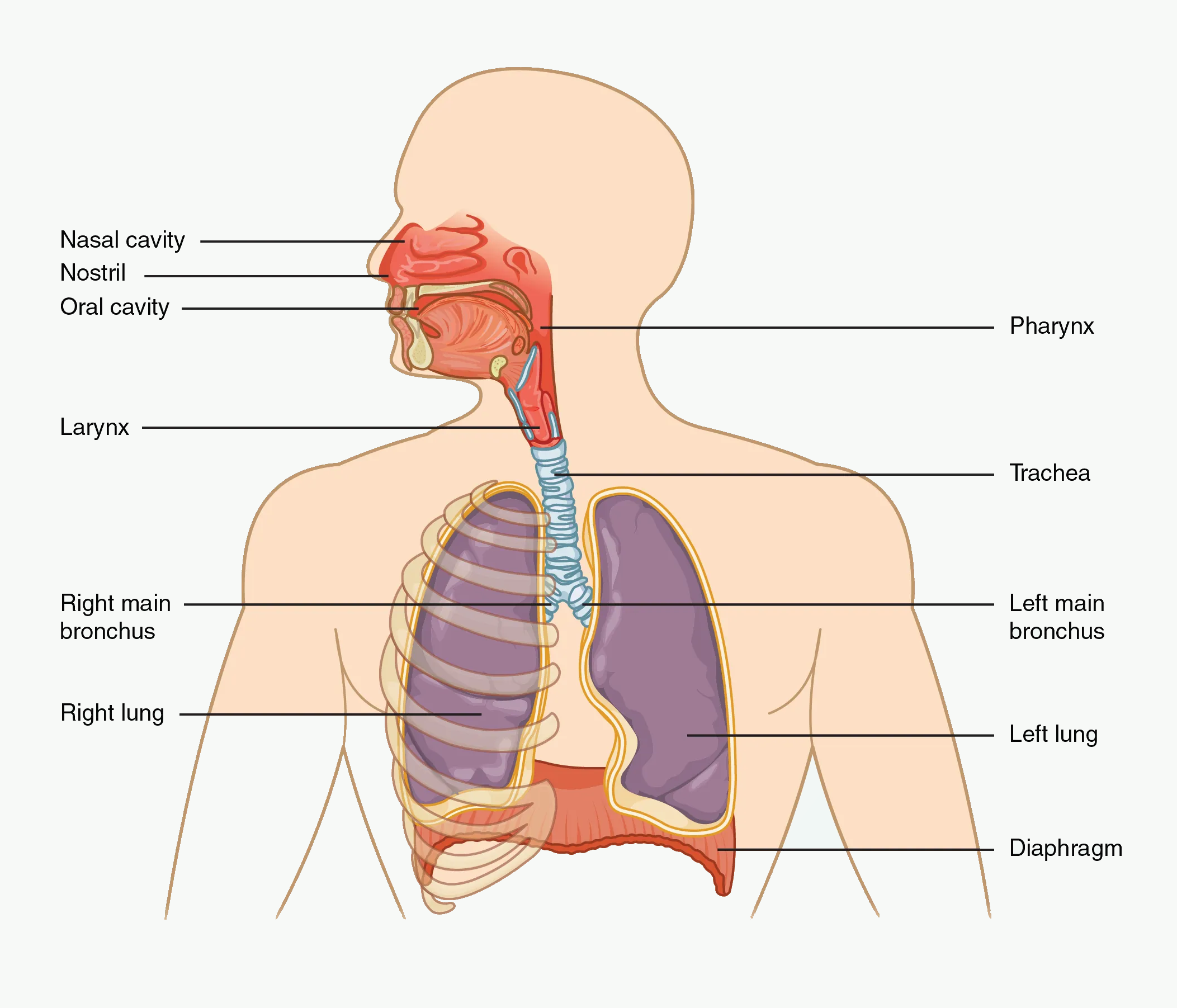
#f7f9f7; anatomical labels and line work unchanged. Source link: openstax.org/books/anatomy-and-physiology/pages/22-1-organs-and-structures-of-the-respiratory-system.How to use this figure: trace gas from nose and mouth to trachea, bronchi, lungs, and diaphragm. Then attach one function to each level: conditioning proximally, conduction through branching airways, and gas exchange distally.
Functional division
For EDAIC Part I, the respiratory tract is best divided by what each region does under stress. Proximal structures conduct, protect, warm, humidify, and filter. Distal structures exchange gas and remain open only if diffusion distance, surface tension, and lung volume are favourable.
Anatomical division
How to use this table: first separate anatomical region from function, then attach the anaesthetic problem: obstruction, aspiration, resistance, secretion retention, atelectasis, or diffusion failure.
| Region | Main structures |
|---|---|
| Upper airway | Nose, nasal cavity, paranasal sinuses, mouth, pharynx |
| Lower airway | Larynx, trachea, bronchi, bronchioles, alveoli |
Some texts place the larynx at the boundary between upper and lower airway. For anaesthetists, it is best treated as the functional gateway between the pharynx and trachea because it is essential for airway protection, phonation, cough, laryngoscopy, intubation, and emergency front-of-neck access.
Functional division
| Zone | Approximate generations | Function |
|---|---|---|
| Conducting zone | 0-16 | Conducts, warms, humidifies, filters; no gas exchange |
| Transitional/respiratory zone | 17-23 | Gas exchange increasingly occurs |
The conducting zone includes the trachea, bronchi, bronchioles, and terminal bronchioles. The respiratory zone includes respiratory bronchioles, alveolar ducts, alveolar sacs, and alveoli.
Major functions of the airway and lung
The airway and lung have both respiratory and non-respiratory functions.
Respiratory functions
- Movement of gas between atmosphere and alveoli.
- Oxygen transfer from alveoli to pulmonary capillary blood.
- Carbon dioxide transfer from pulmonary capillary blood to alveoli.
- Maintenance of alveolar stability through surfactant.
Non-respiratory functions
- Humidification and warming of inspired gas.
- Filtration of particles.
- Mucociliary clearance.
- Cough and sneeze reflexes.
- Immune defence.
- Acid-base regulation through CO₂ excretion.
- Metabolic and endocrine functions, including angiotensin-converting enzyme activity in pulmonary endothelium.
- Blood reservoir and filter for small embolic material.
Quick check: airway map
Where does the conducting zone end?
Reveal answer
At the terminal bronchioles, which are the last purely conducting airways and do not participate in gas exchange.
Where does the respiratory zone begin?
Reveal answer
At the respiratory bronchioles, where alveoli begin to appear in the airway walls and gas exchange starts.
Why is anatomical dead space clinically important?
Reveal answer
Only tidal volume beyond dead space reaches alveoli, so small tidal volumes can move gas visibly while producing poor alveolar ventilation.
EDAIC trap: the upper airway is not just an entry route. It is the conditioning and protection system that anaesthesia commonly disables, especially at the collapsible pharynx.
Upper Airway: Structure and Function
Definition and components
The upper airway consists of air passages above the larynx:
- nose,
- nasal cavity,
- paranasal sinuses,
- mouth,
- pharynx:
- nasopharynx,
- oropharynx,
- laryngopharynx.
Its main function is to conduct air to the lower respiratory tract, but it also filters, warms, humidifies, smells, protects, and participates in speech and swallowing.
Nose and nasal cavity
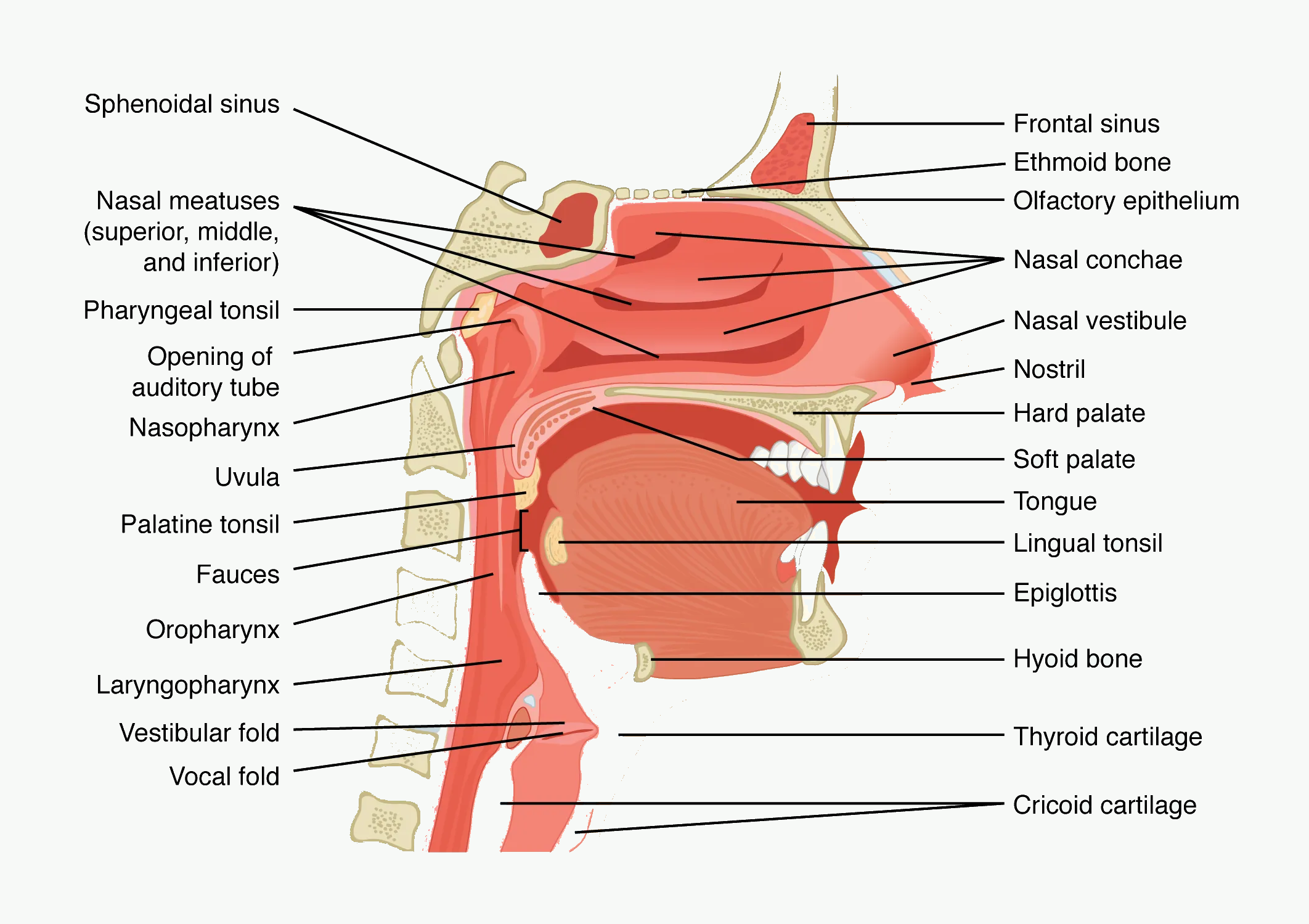
#f7f9f7; anatomical labels and line work unchanged. Source link: openstax.org/books/anatomy-and-physiology/pages/22-1-organs-and-structures-of-the-respiratory-system.How to use this figure: focus on the collapsible pharyngeal segment behind the tongue and soft palate. Sedation removes dilator tone; jaw thrust, oral airways, and CPAP work by moving or splinting this segment.
In exam terms, the nose is an airway conditioning organ. It adds resistance, but it also warms, humidifies, filters, and protects the lower airway. Tracheal tubes and mouth breathing remove much of that protection.
Functions of the nose
| Function | Mechanism |
|---|---|
| Filtration of large particles | Nasal hairs and turbulent airflow |
| Filtration of smaller particles | Mucus traps particles |
| Warming | Rich vascular mucosa transfers heat |
| Humidification | Moist mucosa adds water vapour |
| Olfaction | Olfactory receptors in upper/posterior nasal cavity |
| Airflow regulation | Turbinates increase surface area and turbulence |
| Immune defence | Mucus, IgA, local immune cells |
The nasal turbinates, also called conchae, increase surface area and create turbulent airflow. Turbulence is useful in the nose because it improves contact between inspired gas and warm, moist mucosa. The price is increased resistance.
Anaesthetic relevance
- Nasal breathing adds resistance. The nose contributes substantially to upper airway resistance.
- Nasal obstruction increases work of breathing. This matters during sedation and sleep.
- Nasal mucosa is vascular. Nasal instrumentation can bleed, especially with anticoagulation, trauma, polyps, pregnancy, or inflamed mucosa.
- Vasoconstrictors reduce bleeding. Phenylephrine, xylometazoline, or cocaine-containing preparations are used in some awake nasal intubation techniques.
- Bypassing the nose bypasses humidification. Tracheal intubation exposes the lower airway to dry gases unless humidification is provided.
Mouth
The mouth provides an alternative airway route. It has lower resistance than the nose, but less effective warming, humidification, and filtration.
Anaesthetic relevance:
- Mouth opening is essential for direct laryngoscopy.
- The tongue is a major cause of airway obstruction during anaesthesia.
- Oropharyngeal airways displace the tongue away from the posterior pharyngeal wall.
- Dental status matters because teeth may be damaged during airway manipulation.
Pharynx
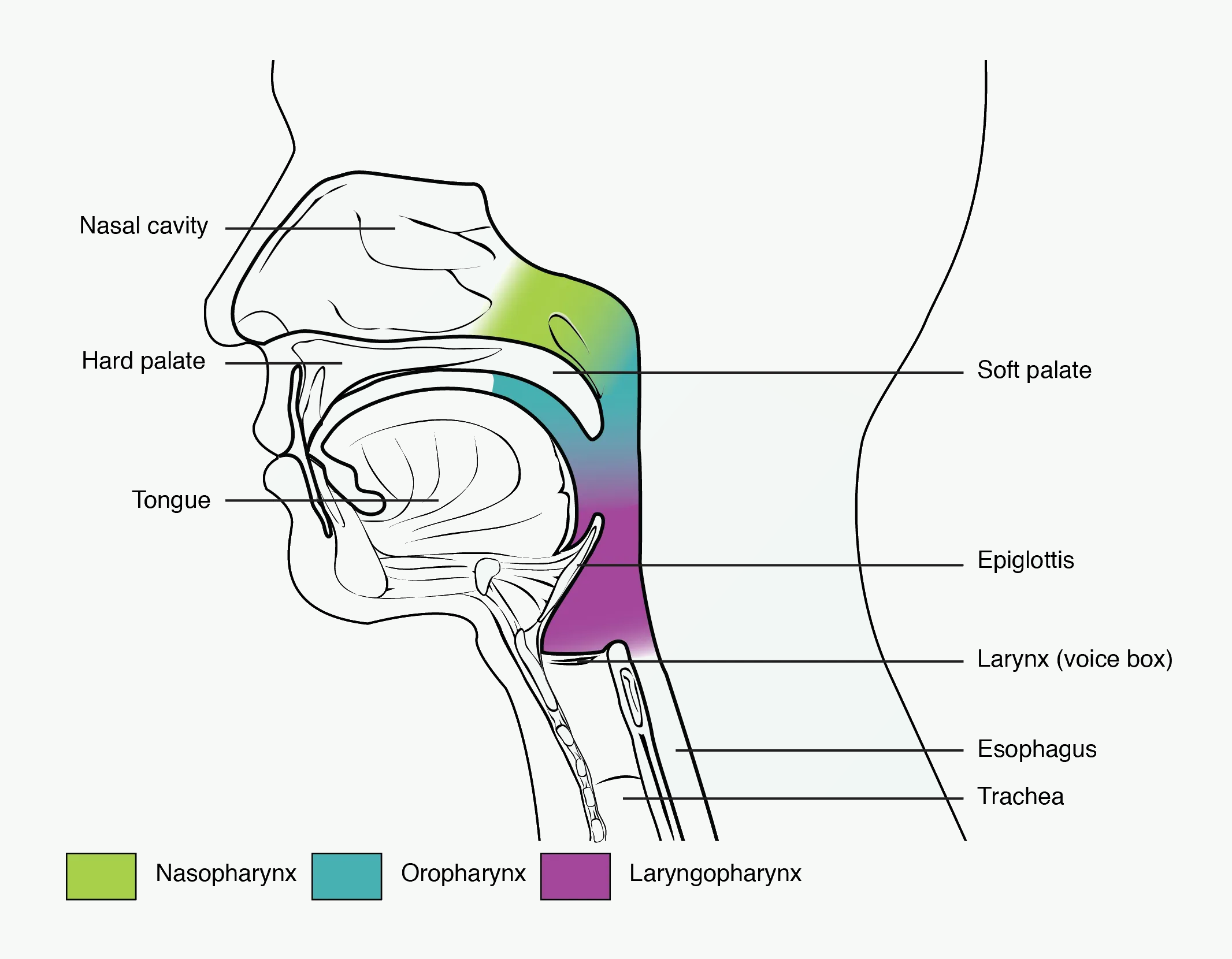
#f7f9f7; anatomical labels and line work unchanged. Source link: openstax.org/books/anatomy-and-physiology/pages/22-1-organs-and-structures-of-the-respiratory-system.How to use this figure: separate nasopharynx, oropharynx, and laryngopharynx. Obstruction, aspiration risk, airway adjunct placement, and laryngoscopy all depend on this shared food-air pathway.
The pharynx is a muscular tube shared by the respiratory and gastrointestinal systems.
It is divided into:
| Region | Extent | Important features |
|---|---|---|
| Nasopharynx | Behind nasal cavity | Eustachian tube opening, adenoids |
| Oropharynx | Behind oral cavity | Tonsils, tongue base |
| Laryngopharynx | From epiglottis to cricoid | Piriform fossae, laryngeal inlet |
The pharynx has several functions:
- conduction of air,
- swallowing,
- speech resonance,
- immune defence through lymphoid tissue,
- protection of the airway during swallowing.
Pharyngeal muscles
Two functional groups are important:
- Pharyngeal constrictors help propel a food bolus during swallowing.
- Pharyngeal dilators maintain airway patency during breathing.
The most important pharyngeal dilator for airway patency is the genioglossus, which pulls the tongue forward and away from the posterior pharyngeal wall.
Why the pharynx collapses
The pharynx is a collapsible muscular tube. It has no rigid cartilage. During inspiration, contraction of the diaphragm creates negative intrathoracic and airway pressure. Negative pressure tends to suck the pharyngeal walls inward.
In the awake patient, pharyngeal dilator muscles activate before and during inspiration, stiffening the airway and preventing collapse.
Important muscles include:
- genioglossus,
- palatal muscles,
- geniohyoid and other hyoid-positioning muscles.
During anaesthesia
General anaesthesia, sedation, opioids, and sleep reduce upper airway dilator muscle tone. The tongue, soft palate, and pharyngeal tissues fall backward. Negative inspiratory pressure worsens collapse.
This explains why airway obstruction is common after induction, especially in:
- obesity,
- obstructive sleep apnoea,
- pregnancy,
- children,
- patients with reduced mandibular space,
- patients with large tongue or tonsils,
- excessive sedation,
- supine positioning.
Why simple airway manoeuvres work
| Manoeuvre/device | Mechanism |
|---|---|
| Head tilt | Aligns airway and reduces soft tissue obstruction |
| Chin lift | Pulls mandible and tongue anteriorly |
| Jaw thrust | Moves mandible, tongue, and epiglottis forward |
| Oropharyngeal airway | Prevents tongue falling against posterior pharynx |
| Nasopharyngeal airway | Bypasses soft palate/tongue obstruction |
| CPAP | Pneumatically splints collapsible pharynx open |
Swallowing and aspiration protection
The airway and oesophagus cross at the pharynx. Protection requires coordination of breathing and swallowing.
During swallowing:
- breathing briefly stops,
- soft palate closes nasopharynx,
- larynx elevates,
- vocal cords close,
- epiglottis helps deflect the bolus,
- upper oesophageal sphincter relaxes,
- pharyngeal constrictors propel the bolus.
Anaesthetic relevance
General anaesthesia impairs:
- consciousness,
- airway reflexes,
- cough,
- swallowing coordination,
- lower oesophageal sphincter tone,
- protective laryngeal closure.
This increases aspiration risk. Patients at increased risk include those with full stomach, bowel obstruction, pregnancy, obesity, reflux, diabetes gastroparesis, trauma, and reduced consciousness.
Quick check: upper-airway collapse and aspiration
Why does the pharynx obstruct so easily during sedation or anaesthesia?
Reveal answer
It is a collapsible muscular tube without cartilage; reduced dilator tone lets the tongue, soft palate, and pharyngeal tissues fall backward.
Why do jaw thrust, airway adjuncts, and CPAP work?
Reveal answer
They move soft tissues away from the posterior pharyngeal wall or splint the collapsible segment open with positive pressure.
Why does anaesthesia increase aspiration risk?
Reveal answer
It depresses consciousness, cough, swallowing coordination, laryngeal reflexes, and protective glottic closure.
EDAIC trap: laryngeal nerve questions are usually functional. Above the cords is internal superior laryngeal sensation; cricothyroid is external superior laryngeal motor; almost everything else motor is recurrent laryngeal.
The Larynx: The Airway Gatekeeper
Position and functions
The larynx lies roughly from C3 to C6. The trachea begins at the lower border of the cricoid cartilage, around C6.
Functions:
- airway protection,
- phonation,
- cough generation,
- regulation of airflow resistance,
- contribution to physiological PEEP,
- passage for tracheal intubation,
- landmark for emergency cricothyroidotomy.
Laryngeal cartilages
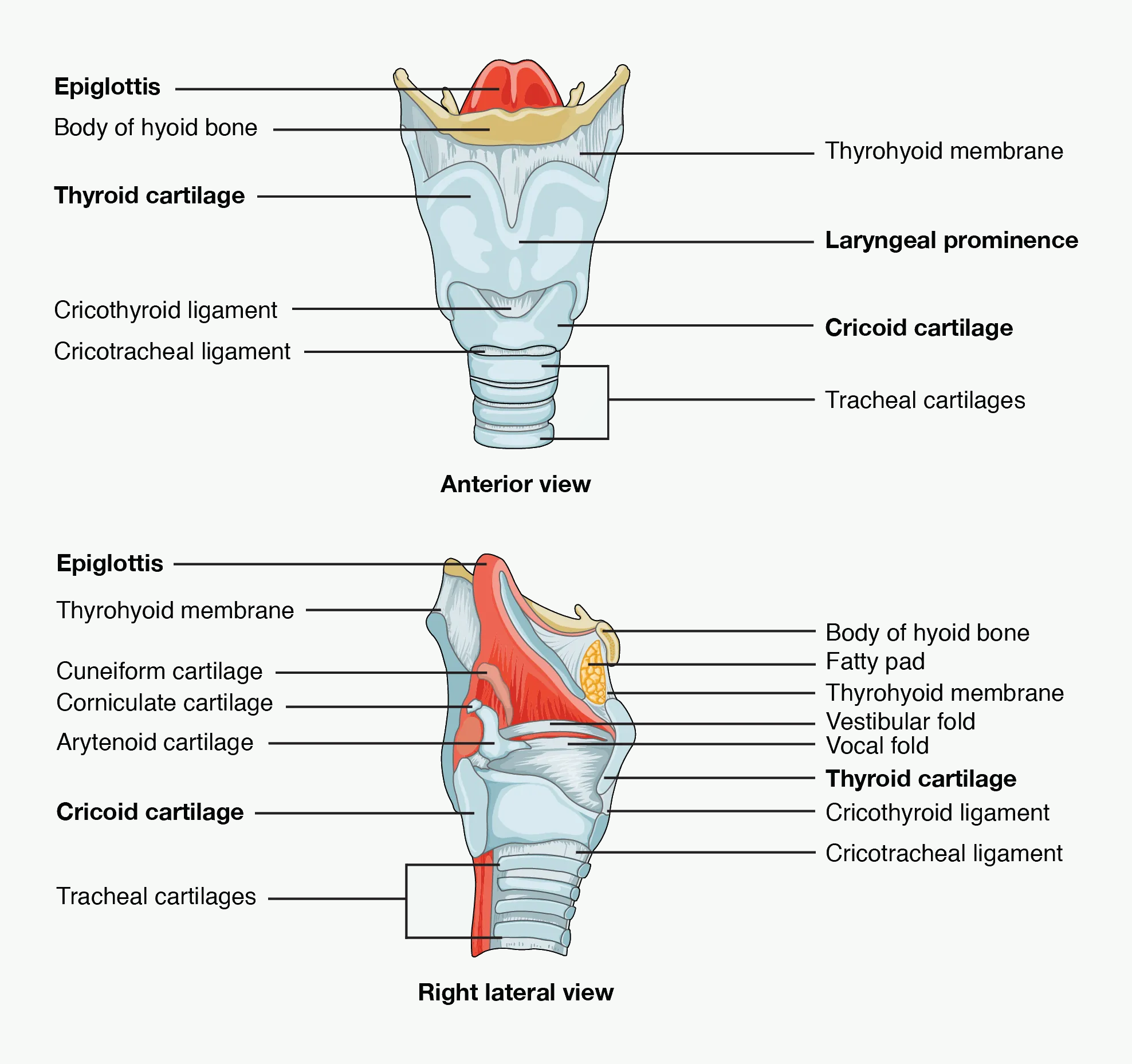
#f7f9f7; anatomical labels and line work unchanged. Source link: openstax.org/books/anatomy-and-physiology/pages/22-1-organs-and-structures-of-the-respiratory-system.How to use this figure: identify epiglottis, vocal folds, thyroid cartilage, cricoid cartilage, and the cricothyroid membrane. These landmarks connect airway protection, laryngospasm, intubation, and emergency front-of-neck access.
There are nine cartilages: three unpaired and three paired.
| Type | Cartilage | Key point |
|---|---|---|
| Unpaired | Epiglottis | Leaf-shaped, helps protect laryngeal inlet |
| Unpaired | Thyroid | Largest; forms laryngeal prominence |
| Unpaired | Cricoid | Complete ring; signet-ring shape; below thyroid cartilage |
| Paired | Arytenoid | Attach to vocal ligaments and move vocal cords |
| Paired | Corniculate | On aryepiglottic folds |
| Paired | Cuneiform | Support aryepiglottic folds |
Vallecula
The vallecula is the space between the base of the tongue and the epiglottis. In adult direct laryngoscopy with a Macintosh blade, the tip is placed in the vallecula to lift the epiglottis indirectly.
Cricoid cartilage and cricothyroid membrane
The cricoid cartilage is the only complete ring in the airway. The cricothyroid membrane lies between the thyroid and cricoid cartilages and is the site for emergency front-of-neck access.
Vocal cords and glottis
The true vocal cords are formed by vocal ligaments covered by mucosa. They run from the thyroid cartilage anteriorly to arytenoid cartilages posteriorly.
The opening between the vocal cords is the rima glottidis.
Movement during breathing
- During inspiration, the vocal cords abduct to reduce resistance.
- During expiration, the cords adduct slightly.
Slight expiratory adduction creates a small physiological PEEP, around 3-4 cmH₂O. This helps maintain functional residual capacity, reduce small-airway collapse, assist cough, and support phonation.
Intubation and loss of physiological PEEP
When a patient is intubated, the endotracheal tube holds the glottis open and bypasses normal cord function. Physiological PEEP from glottic adduction is lost. This contributes to atelectasis and ventilation-perfusion mismatch unless external PEEP is applied.
This is why applying about 3-5 cmH₂O of PEEP during controlled ventilation often reproduces a normal physiological effect rather than being a purely artificial intervention.
Laryngeal muscles
Key intrinsic muscles
| Muscle | Function | Nerve |
|---|---|---|
| Posterior cricoarytenoid | Abducts vocal cords | Recurrent laryngeal nerve |
| Lateral cricoarytenoid | Adducts vocal cords | Recurrent laryngeal nerve |
| Transverse/oblique arytenoids | Adduct arytenoids | Recurrent laryngeal nerve |
| Thyroarytenoid/vocalis | Relaxes/adjusts vocal cord tension | Recurrent laryngeal nerve |
| Cricothyroid | Tenses vocal cords | External branch of superior laryngeal nerve |
High-yield facts:
- Posterior cricoarytenoid is the only abductor of the vocal cords.
- Cricothyroid is the only intrinsic laryngeal muscle supplied by the external branch of the superior laryngeal nerve.
- All other intrinsic laryngeal muscles are supplied by the recurrent laryngeal nerve.
Laryngeal innervation
The larynx is supplied by branches of the vagus nerve.
| Nerve | Sensory supply | Motor supply |
|---|---|---|
| Internal branch of superior laryngeal nerve | Above vocal cords, including epiglottis and laryngeal inlet | None |
| External branch of superior laryngeal nerve | Minimal sensory | Cricothyroid muscle |
| Recurrent laryngeal nerve | Below vocal cords | All intrinsic laryngeal muscles except cricothyroid |
Clinical relevance
- Internal superior laryngeal nerve block anaesthetises the larynx above the cords.
- Transtracheal local anaesthetic through the cricothyroid membrane anaesthetises trachea and below the cords by coughing local anaesthetic upward.
- Recurrent laryngeal nerve injury may cause hoarseness, aspiration, or airway obstruction depending on whether unilateral or bilateral.
- Bilateral recurrent laryngeal nerve palsy can cause severe airway obstruction if cords lie near the midline.
- Left recurrent laryngeal nerve has a longer intrathoracic course and is vulnerable to thoracic pathology.
Laryngeal reflexes
The larynx is highly reflexogenic because it protects the lungs from aspiration.
Important reflexes:
| Reflex | Stimulus | Response |
|---|---|---|
| Cough | Irritation of larynx/trachea/bronchi | Deep inspiration, glottic closure, forceful expiration |
| Laryngospasm | Strong laryngeal stimulation, secretions, blood, light anaesthesia | Reflex vocal cord closure |
| Apnoea during swallowing | Swallowing | Brief interruption of breathing |
Laryngospasm
Laryngospasm is reflex closure of the vocal cords. It is more likely with:
- light anaesthesia,
- airway secretions,
- blood in pharynx,
- airway instrumentation,
- children,
- recent upper respiratory infection,
- extubation in an irritable airway.
It can cause complete airway obstruction, negative-pressure pulmonary oedema, hypoxaemia, bradycardia, and cardiac arrest if untreated.
Quick check: laryngeal protection and innervation
Which intrinsic laryngeal muscle abducts the vocal cords?
Reveal answer
Posterior cricoarytenoid is the only vocal cord abductor, and it is supplied by the recurrent laryngeal nerve.
Which intrinsic laryngeal muscle is the superior-laryngeal-nerve exception?
Reveal answer
Cricothyroid is supplied by the external branch of the superior laryngeal nerve; most other intrinsic muscles are recurrent laryngeal nerve.
What makes laryngospasm dangerous?
Reveal answer
Reflex vocal cord closure can become complete obstruction, causing hypoxaemia, negative-pressure pulmonary oedema, bradycardia, and arrest.
EDAIC trap: do not treat lower-airway branching as a diagram only. The right main bronchus explains tube malposition and aspiration; bronchioles explain bronchospasm and collapse because they have no cartilage.
Lower Airways and the Tracheobronchial Tree
Trachea
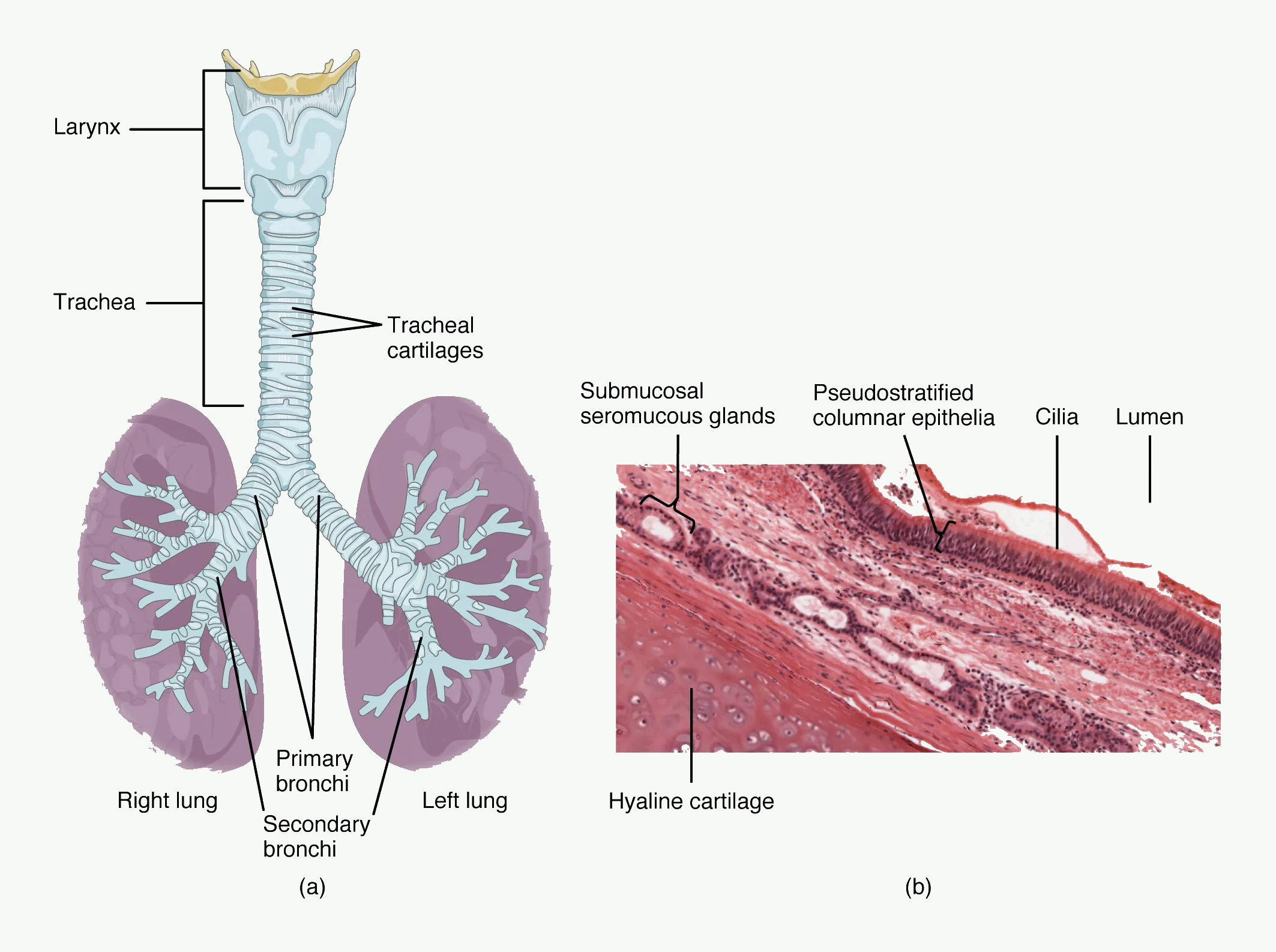
#f7f9f7; anatomical labels and line work unchanged. Source link: openstax.org/books/anatomy-and-physiology/pages/22-1-organs-and-structures-of-the-respiratory-system.How to use this figure: notice C-shaped cartilage, posterior membranous trachea, and proximity to the oesophagus. Tube cuff pressure, tracheomalacia, and airway injury all become easier to reason through from this structure.
The trachea begins at the cricoid cartilage around C6 and extends to the carina around T4/T5 in adults, where it divides into right and left main bronchi.
Key features:
- C-shaped cartilaginous rings support the anterior and lateral walls.
- Posterior wall contains trachealis muscle.
- Lined by pseudostratified ciliated columnar epithelium with goblet cells.
- Contains mucus glands and immune cells.
Anaesthetic relevance
- Endotracheal tubes can irritate the trachea and provoke cough or bronchospasm.
- Cuff pressure must be controlled to avoid mucosal ischaemia.
- Carina stimulation is very irritating and can cause coughing or sympathetic response.
- Tube position matters: too deep often enters the right main bronchus.
Bronchi
The trachea divides into right and left main bronchi.
Right main bronchus
The right main bronchus is generally:
- wider,
- shorter,
- more vertical.
Clinical relevance:
- Aspirated material more often enters the right bronchial tree.
- A tracheal tube advanced too far commonly enters the right main bronchus.
- Right upper lobe obstruction can still occur depending on tube position.
Bronchial structure
As bronchi divide:
- cartilage becomes less regular,
- smooth muscle becomes more important,
- submucosal glands decrease,
- airway diameter becomes smaller,
- total cross-sectional area increases.
Bronchioles
Bronchioles are small airways without cartilage.
Features:
- no cartilage,
- prominent smooth muscle,
- fewer goblet cells,
- ciliated epithelium becomes simpler,
- terminal bronchioles are the last purely conducting airways.
Anaesthetic relevance
Because bronchioles lack cartilage, their calibre is strongly influenced by:
- smooth muscle tone,
- lung volume,
- surrounding parenchymal traction,
- airway inflammation,
- mucus plugging,
- bronchospasm,
- intrathoracic pressure.
Small-airway collapse is common when lung volume falls, especially under general anaesthesia, obesity, pregnancy, and supine positioning.
Conducting zone
The conducting zone extends from trachea to terminal bronchioles.
Functions:
- conduct gas,
- warm and humidify inspired air,
- filter particles,
- distribute ventilation,
- contribute to airway resistance,
- provide anatomical dead space,
- clear mucus by mucociliary transport.
There is no gas exchange in the conducting zone because the airway walls are too thick and not closely associated with pulmonary capillaries.
Anatomical dead space
Anatomical dead space is the volume of conducting airway that does not participate in gas exchange.
Approximate adult value:
- about 150 mL,
- or 2 mL/kg.
This matters because alveolar ventilation depends on tidal volume minus dead space:
Alveolar ventilation = respiratory rate × (tidal volume - dead space)
A patient taking small tidal volumes may move gas in and out of the mouth but ventilate alveoli poorly.
Respiratory zone
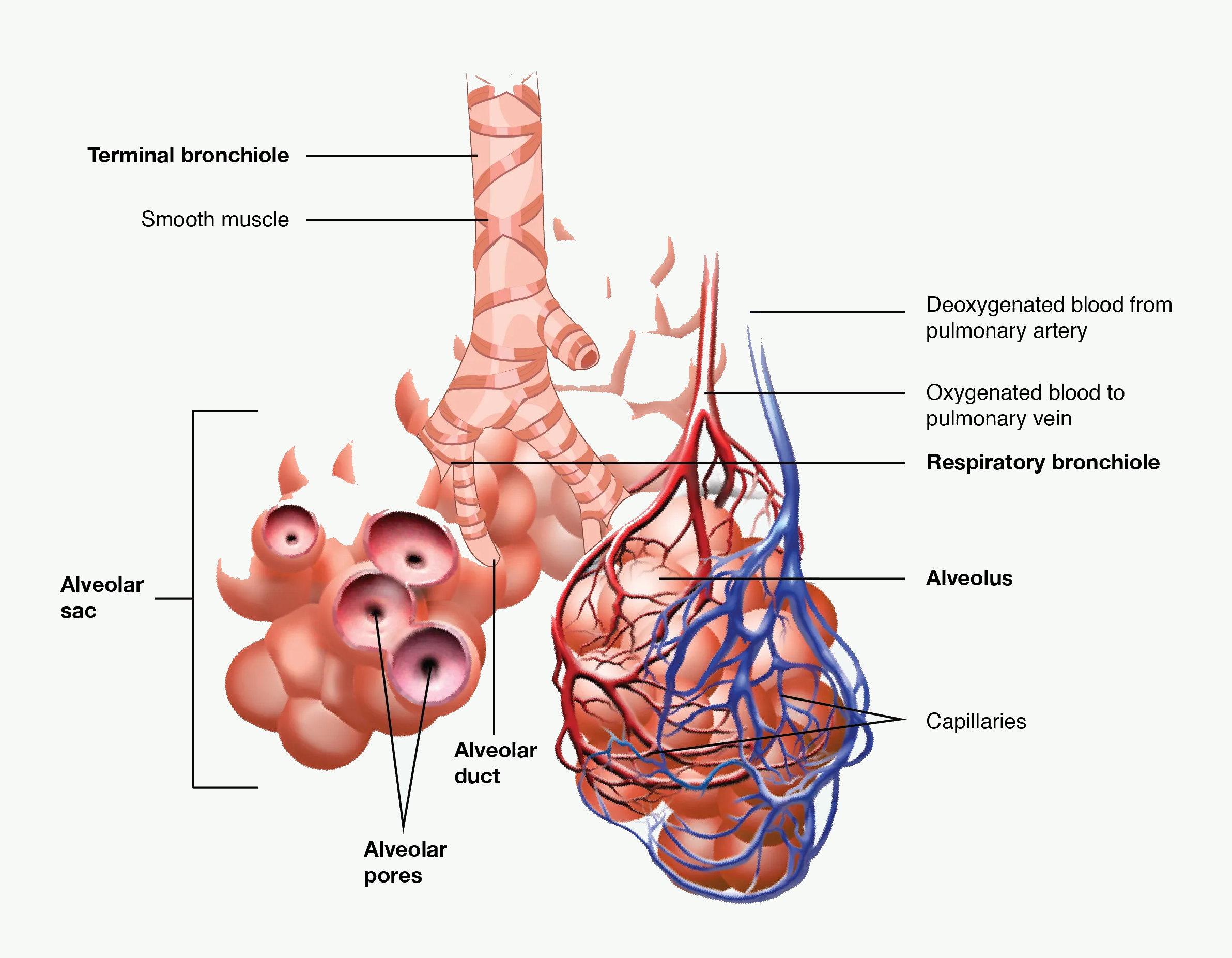
#f7f9f7; anatomical labels and line work unchanged. Source link: openstax.org/books/anatomy-and-physiology/pages/22-1-organs-and-structures-of-the-respiratory-system.How to use this figure: terminal bronchiole is the end of the conducting zone; respiratory bronchiole begins the respiratory zone. Smooth muscle without cartilage explains small-airway narrowing and collapse.
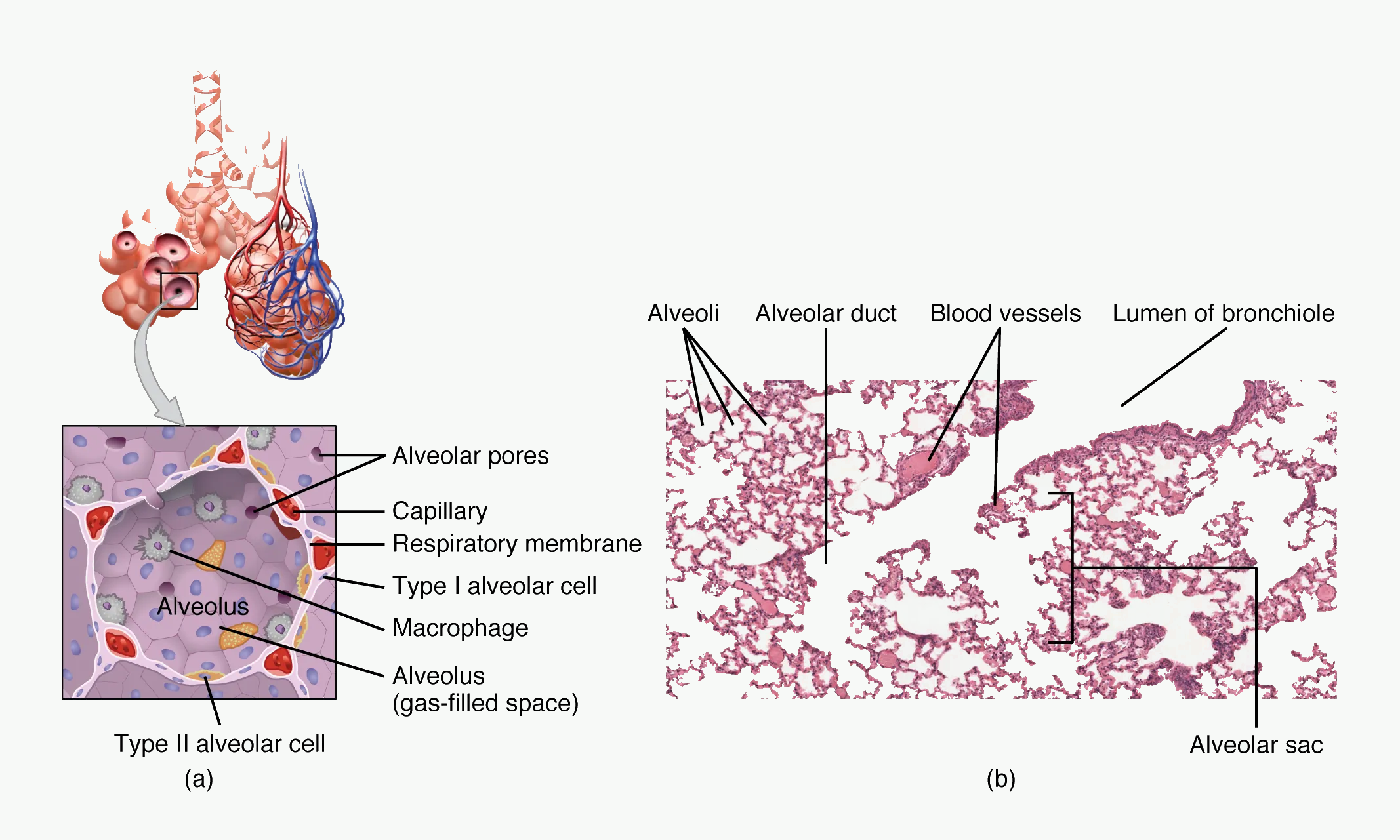
#f7f9f7; anatomical labels, micrograph, and line work unchanged. Source link: openstax.org/books/anatomy-and-physiology/pages/22-1-organs-and-structures-of-the-respiratory-system.How to use this figure: connect type I pneumocytes with thin diffusion distance, type II pneumocytes with surfactant and repair, macrophages with defence, and capillaries with rapid gas transfer.
The respiratory zone begins where alveoli appear in airway walls.
It includes:
- respiratory bronchioles,
- alveolar ducts,
- alveolar sacs,
- alveoli.
Functions:
- oxygen diffusion into blood,
- carbon dioxide diffusion into alveoli,
- surfactant production,
- immune surveillance by alveolar macrophages.
The respiratory zone is specialised for diffusion:
- enormous surface area,
- very thin barrier,
- dense pulmonary capillary network,
- short diffusion distance,
- large partial-pressure gradients.
Airway generations
A useful model is Weibel's airway generation model.
| Generation | Structure | Main function |
|---|---|---|
| 0 | Trachea | Conducting |
| 1-3 | Main/lobar/segmental bronchi | Conducting |
| 4-16 | Smaller bronchi and terminal bronchioles | Conducting |
| 17-19 | Respiratory bronchioles | Transitional/gas exchange begins |
| 20-22 | Alveolar ducts | Gas exchange |
| 23 | Alveolar sacs | Gas exchange |
Exam point:
- Terminal bronchioles are the last part of the conducting zone.
- Respiratory bronchioles are the first part of the respiratory zone.
Structural changes down the airway
| Feature | Trachea/large bronchi | Bronchioles | Alveoli |
|---|---|---|---|
| Cartilage | Present | Absent | Absent |
| Smooth muscle | Present | Important | Minimal around openings |
| Epithelium | Pseudostratified ciliated columnar | Ciliated cuboidal | Squamous type I cells |
| Goblet cells | Many | Fewer | Absent |
| Cilia | Present | Present until distal bronchioles | Absent in alveoli |
| Gas exchange | None | None until respiratory bronchioles | Main function |
| Main problem clinically | Obstruction, secretions, intubation | Bronchospasm, collapse, mucus plugging | Collapse, oedema, diffusion impairment |
Quick check: lower-airway structure
Why is the right main bronchus a common site for aspiration or tube malposition?
Reveal answer
It is generally wider, shorter, and more vertical, so aspirated material and overly deep tracheal tubes tend to enter it.
Why are bronchioles vulnerable to collapse and bronchospasm?
Reveal answer
They lack cartilage, so calibre depends heavily on smooth muscle tone, lung volume, radial traction, mucus, oedema, and intrathoracic pressure.
What structural change makes alveoli suited for diffusion?
Reveal answer
They have a huge surface area, thin type I pneumocytes, close capillaries, and a very short diffusion distance.
EDAIC trap: resistance is a radius problem before it is a ventilator problem. Small oedema, secretions, bronchospasm, kinking, or a narrow tube can cause a large work-of-breathing penalty.
Airway Resistance and Flow
Why airway radius matters
For laminar flow, Poiseuille's law states:
Resistance proportional to 1 / radius^4
This means a small decrease in radius produces a large increase in resistance.
Example:
If airway radius halves, resistance increases by 16 times.
This is crucial in:
- bronchospasm,
- airway oedema,
- secretions,
- small endotracheal tubes,
- paediatric airway obstruction,
- upper airway collapse.
Laminar, turbulent, and transitional flow
| Flow type | Features | Where common |
|---|---|---|
| Laminar | Smooth layers; resistance predictable by Poiseuille's law | Small airways at low flow |
| Turbulent | Chaotic flow; resistance rises greatly with flow | Nose, pharynx, trachea, high flow states |
| Transitional | Mixed pattern | Branch points |
Turbulence increases with:
- high flow,
- large airway diameter,
- high gas density,
- irregular airway shape,
- sharp bends and branching,
- obstruction.
Heliox reduces resistance in turbulent flow because helium has low density. It may improve airflow in upper airway obstruction, severe asthma, or narrowed airways, but it does not treat the underlying cause.
Endotracheal tube resistance
An endotracheal tube is narrower and longer than the normal upper airway route, so it increases resistance. Resistance is especially important with small tubes.
Clinical implications:
- A 6.0 mm tube has much greater resistance than an 8.0 mm tube.
- Work of breathing increases during spontaneous ventilation through small tubes.
- Secretions or kinking further increase resistance.
- In children, 1 mm of oedema causes a major proportional reduction in radius.
Quick check: resistance and tube physiology
Why does a small reduction in radius matter so much?
Reveal answer
For laminar flow, resistance varies inversely with the fourth power of radius, so halving radius increases resistance about sixteen-fold.
When is endotracheal tube resistance especially important?
Reveal answer
During spontaneous breathing or weaning through small, kinked, or secretion-narrowed tubes, because the patient must generate the pressure to overcome that resistance.
Why can heliox reduce work in selected obstructed airways?
Reveal answer
Its lower density reduces turbulent-flow resistance, but it is a bridge and does not treat the cause of obstruction.
EDAIC trap: humidification failures are slow but important. A tube bypasses the nose and pharynx; dry gas thickens secretions, impairs cilia, raises resistance, and can block the tube.
Humidification and Airway Conditioning
Normal humidification
By the time inspired gas reaches the alveoli, it is normally:
- warmed to body temperature,
- fully saturated with water vapour,
- filtered of many particles.
At 37 degrees C, saturated water vapour pressure is approximately 47 mmHg or 6.3 kPa.
The nose and upper airway normally provide most of this conditioning.
What happens when the upper airway is bypassed?
Tracheal intubation bypasses the nose, mouth, and much of the pharynx.
Dry, cold gas delivered to the trachea may cause:
- thick secretions,
- impaired ciliary function,
- mucus plugging,
- atelectasis,
- increased airway resistance,
- epithelial injury,
- heat and water loss,
- tube blockage.
This is why humidification is required during prolonged ventilation.
Humidification devices
| Device | Function |
|---|---|
| Heat and moisture exchanger | Conserves patient's expired heat and moisture |
| Heated humidifier | Adds active heat and water vapour |
Heat and moisture exchangers are simple and common but may increase dead space and resistance. Heated humidifiers are useful when secretions are thick, ventilation is prolonged, or leak/high flow reduces HME effectiveness.
EDAIC trap: suction removes visible secretions but does not replace mucociliary clearance. The exam often links dry gas, hypothermia, smoking, dehydration, and intubation to impaired ciliary function.
Mucociliary Clearance
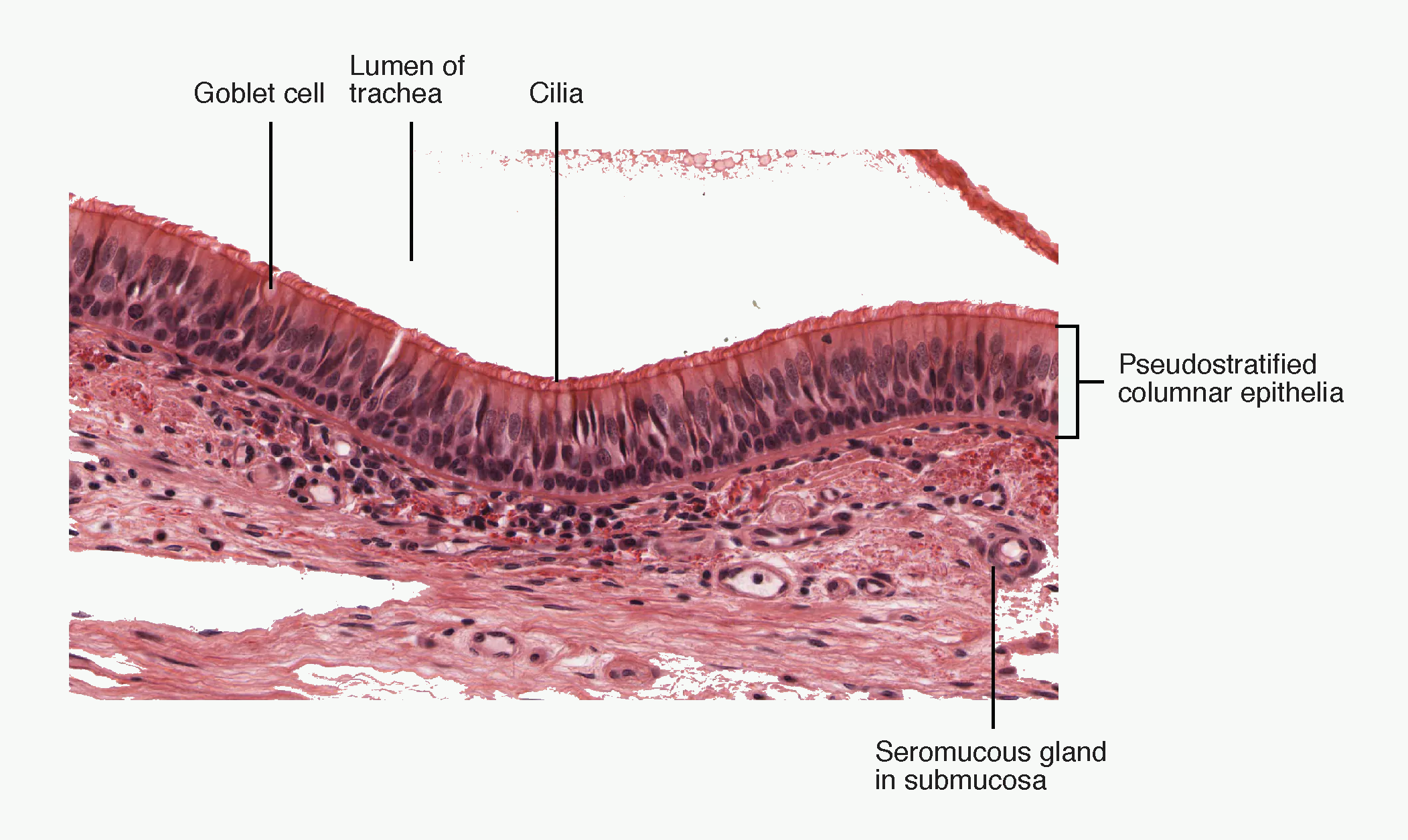
#f7f9f7; anatomical labels and line work unchanged. Source link: openstax.org/books/anatomy-and-physiology/pages/22-1-organs-and-structures-of-the-respiratory-system.How to use this figure: relate goblet cells, cilia, and mucus layers to the mucociliary escalator. Dry gas, smoking, infection, intubation, and dehydration impair exactly this mechanism.
Definition
Mucociliary clearance is the movement of mucus and trapped particles from the lower respiratory tract toward the pharynx by coordinated ciliary beating.
It is often called the mucociliary escalator.
Structure
The conducting airways are lined by respiratory epithelium containing:
- ciliated epithelial cells,
- goblet cells,
- submucosal glands,
- mucus layer,
- periciliary sol layer,
- immune cells.
Mucus has two functional layers:
| Layer | Function |
|---|---|
| Gel layer | Sticky upper layer traps particles and microbes |
| Sol/periciliary layer | Watery lower layer allows cilia to beat effectively |
Cilia beat in a coordinated direction toward the pharynx. Mucus is swallowed or expectorated.
Functions
Mucociliary clearance removes:
- dust,
- pathogens,
- cell debris,
- inhaled particles,
- excess secretions.
It protects the distal lung from infection and obstruction.
Factors impairing mucociliary clearance
| Factor | Effect |
|---|---|
| Smoking | Damages cilia, increases mucus production |
| Dry gases | Thickens secretions, slows cilia |
| Endotracheal tube | Bypasses upper airway, impairs cough and cilia |
| General anaesthesia | Reduces cough, alters clearance |
| Hypothermia | Slows ciliary activity |
| Dehydration | Thickens mucus |
| Infection/inflammation | Damages epithelium, increases secretions |
| High inspired oxygen for prolonged periods | May impair epithelial function |
| Anticholinergic drugs | Reduce secretions but may thicken mucus |
| Cystic fibrosis | Abnormally viscous secretions |
| Primary ciliary dyskinesia | Defective ciliary movement |
Anaesthetic relevance
Ventilated patients are vulnerable to secretion retention because:
- the upper airway is bypassed,
- cough is reduced or abolished,
- humidification may be inadequate,
- immobility promotes atelectasis,
- suctioning may injure mucosa,
- infection risk increases.
Good airway care requires humidification, suctioning when needed, hydration, physiotherapy, appropriate PEEP, and early mobilisation where possible.
Quick check: humidification and clearance
What happens when the upper airway is bypassed for a long time?
Reveal answer
Dry cold gas can thicken secretions, slow cilia, injure epithelium, increase resistance, promote mucus plugs, and cause atelectasis.
What does mucociliary clearance require?
Reveal answer
A hydrated mucus layer, functioning cilia, appropriate airway humidity, intact epithelium, and enough cough or suction support to clear larger secretions.
Why are ventilated patients prone to retained secretions?
Reveal answer
The tube bypasses conditioning, reduces cough efficiency, irritates mucosa, increases infection risk, and often combines with immobility and inadequate humidification.
Cough and Airway Defence
Cough reflex
Cough is a protective reflex that clears the airway.
Receptors
Cough receptors are found in:
- larynx,
- trachea,
- carina,
- large bronchi,
- pleura,
- external auditory canal in some individuals.
Afferent pathway is mainly via the vagus nerve to the medulla.
Phases of cough
- Inspiratory phase - deep inspiration increases lung volume.
- Compression phase - glottis closes; expiratory muscles contract; intrathoracic pressure rises.
- Expulsive phase - glottis opens suddenly; high-velocity airflow expels mucus or foreign material.
Anaesthetic relevance
Cough requires:
- consciousness or brainstem reflex integrity,
- intact laryngeal sensation,
- glottic closure and opening,
- adequate respiratory muscle strength,
- adequate lung volume,
- unobstructed airway.
Anaesthesia, opioids, neuromuscular blockade, stroke, high spinal cord injury, critical illness weakness, and tracheostomy can all impair cough.
Other airway defence mechanisms
| Defence | Role |
|---|---|
| Nasal hairs and turbinates | Trap large particles |
| Mucus | Traps particles and microbes |
| Cilia | Move mucus toward pharynx |
| Cough | Clears large airway material |
| Sneeze | Clears nasal irritants |
| Secretory IgA | Mucosal immune defence |
| Alveolar macrophages | Phagocytose particles in alveoli |
| Surfactant proteins A and D | Innate immune roles |
| Laryngospasm | Prevents entry of material into trachea, but may obstruct airway dangerously |
Alveoli and the Gas Exchange Surface
Alveolar structure
Alveoli are tiny air sacs specialised for gas exchange. There are hundreds of millions of alveoli, producing a very large surface area for diffusion.
Important cells:
| Cell | Function |
|---|---|
| Type I pneumocyte | Thin squamous cell; main gas exchange surface |
| Type II pneumocyte | Produces surfactant; progenitor cell for alveolar epithelium |
| Alveolar macrophage | Immune defence and particle clearance |
| Capillary endothelial cell | Blood side of gas exchange barrier |
Type I pneumocytes cover most of the alveolar surface area. Type II pneumocytes are more cuboidal, produce surfactant, and help repair alveolar injury.
Alveolar-capillary membrane
The diffusion barrier includes:
- surfactant layer,
- alveolar epithelial cell,
- epithelial basement membrane,
- interstitial space,
- capillary basement membrane,
- capillary endothelial cell,
- plasma,
- red cell membrane.
Gas exchange is efficient because the barrier is extremely thin and the capillary network is dense.
This becomes more important in later modules on oxygen transport, CO₂ transport, and alveolar diffusion.
Alveolar pores and collateral ventilation
Alveoli communicate through small pores, often called pores of Kohn. Additional collateral channels may exist between bronchioles and alveoli.
Collateral ventilation can help ventilate alveoli distal to partial obstruction, but it can also spread infection or air leak.
EDAIC trap: surfactant is not only a neonatal topic. It is the mechanism that links Laplace law, compliance, atelectasis, shunt, ARDS, aspiration, and anaesthesia-related lung collapse.
Surfactant
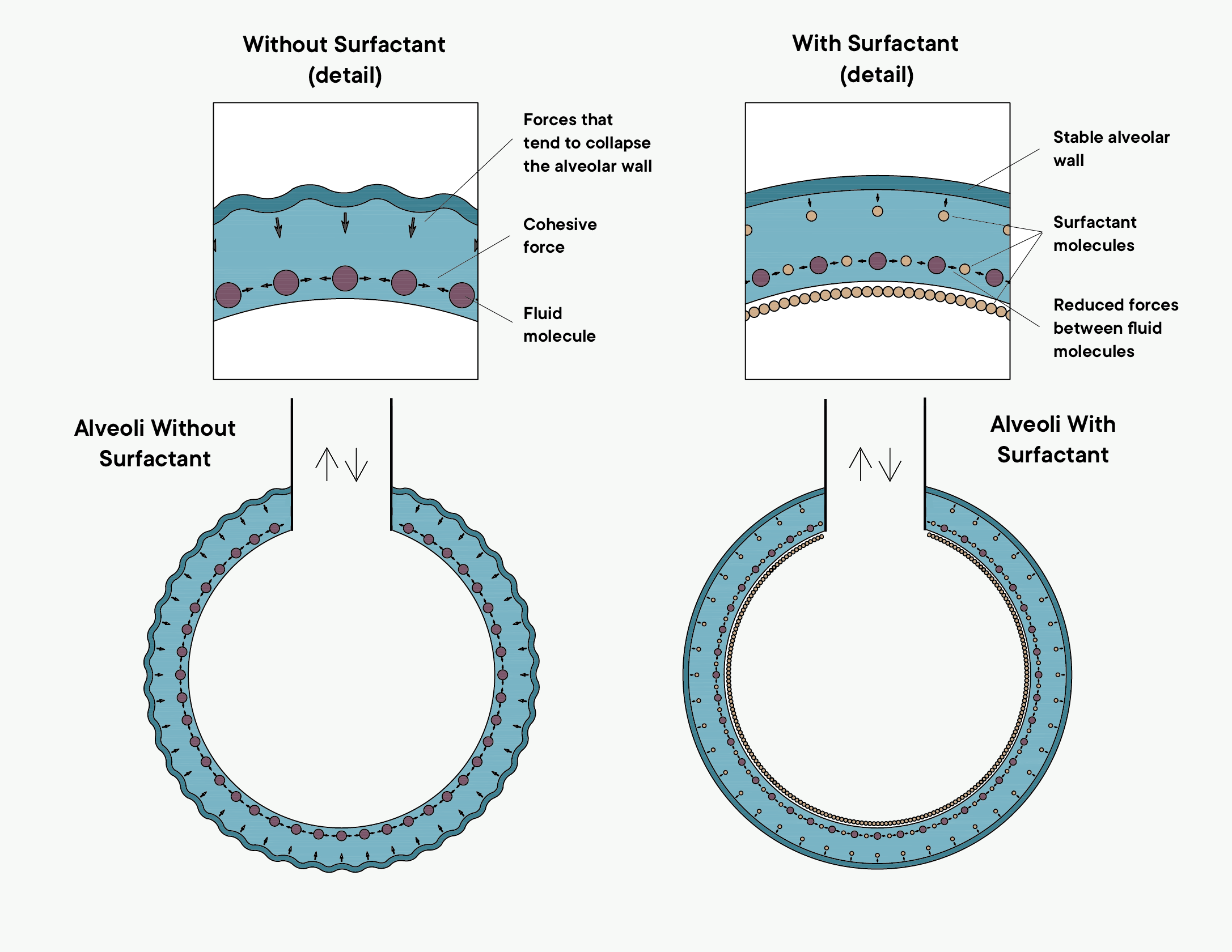
#f7f9f7; diagram elements, labels, colours, and line work unchanged. Source link: commons.wikimedia.org/wiki/File:Diagram_of_Surfactant_2_.png.How to use this figure: compare high surface tension without surfactant with stabilised alveoli when surfactant is present. This is the visual version of Laplace law and neonatal respiratory distress.
Definition
Pulmonary surfactant is a mixture of phospholipids and proteins produced by type II pneumocytes that reduces surface tension at the air-liquid interface in alveoli.
A good exam definition:
Surfactant is a phospholipid-protein mixture secreted by type II pneumocytes that reduces alveolar surface tension, increases compliance, stabilises alveoli, reduces work of breathing, and helps keep alveoli dry.
Composition
Surfactant contains:
- phospholipids,
- neutral lipids,
- surfactant proteins.
The most important phospholipid is:
- dipalmitoylphosphatidylcholine, abbreviated DPPC.
Important surfactant proteins:
| Protein | Main role |
|---|---|
| SP-A | Innate immunity and surfactant regulation |
| SP-B | Surfactant spreading and function |
| SP-C | Surfactant spreading and stability |
| SP-D | Innate immunity |
Production and fetal development
Surfactant is produced by type II pneumocytes.
High-yield developmental points:
- Type II pneumocytes begin producing surfactant from around 24 weeks' gestation.
- Functional maturity increases later in gestation.
- Full lung maturation is usually closer to 35 weeks.
- Antenatal corticosteroids increase fetal surfactant production when preterm delivery is expected.
Stimuli increasing surfactant production include:
- alveolar stretch,
- glucocorticoids,
- catecholamines,
- thyroid hormones.
Surface tension problem
Alveoli are lined by a thin liquid layer. Water molecules attract each other, producing surface tension. Surface tension tends to collapse alveoli and draw fluid into them.
If there were no surfactant, the lungs would be stiff, unstable, and wet.
Laplace's law
For a spherical alveolus:
P = 2T / r
where:
- P = pressure needed to keep the alveolus open,
- T = surface tension,
- r = radius.
If surface tension were constant, small alveoli would need higher pressure to stay open than large alveoli. Therefore, small alveoli would empty into large alveoli and collapse.
Surfactant solves this problem because it reduces surface tension more in small alveoli than in large alveoli. As an alveolus becomes smaller, surfactant molecules become more concentrated at the surface, reducing surface tension further.
Functions of surfactant
| Function | Explanation |
|---|---|
| Reduces surface tension | Decreases collapsing force in alveoli |
| Increases compliance | Less pressure needed to inflate lungs |
| Reduces work of breathing | Particularly important in neonates and respiratory disease |
| Stabilises small alveoli | Prevents small alveoli emptying into larger ones |
| Prevents atelectasis | Helps maintain alveolar recruitment at low lung volumes |
| Keeps alveoli dry | Reduces fluid transudation into alveoli |
| Supports immunity | Surfactant proteins contribute to innate defence |
Surfactant and compliance
Compliance is the change in volume for a given change in pressure:
Compliance = ΔV / ΔP
By lowering surface tension, surfactant increases lung compliance. A more compliant lung requires less pressure and less work to inflate.
When surfactant is deficient or inactivated:
- compliance falls,
- work of breathing rises,
- alveoli collapse,
- oxygenation worsens,
- pulmonary oedema may develop,
- ventilation becomes uneven.
Surfactant deficiency and dysfunction
Infant respiratory distress syndrome
Premature neonates may have inadequate surfactant. Consequences:
- low compliance,
- atelectasis,
- increased work of breathing,
- hypoxaemia,
- respiratory failure,
- diffuse alveolar collapse.
Prevention/treatment:
- antenatal corticosteroids when preterm delivery is expected,
- CPAP or ventilatory support,
- exogenous surfactant therapy in selected neonates.
ARDS
In acute respiratory distress syndrome, surfactant may be inactivated by inflammation, oedema fluid, plasma proteins, and epithelial injury.
Consequences:
- stiff lungs,
- widespread atelectasis,
- shunt,
- severe hypoxaemia,
- reduced compliance.
Near-drowning and aspiration
Surfactant can be washed out or inactivated, causing atelectasis, low compliance, and pulmonary oedema.
General anaesthesia
General anaesthesia promotes atelectasis through:
- reduced FRC,
- loss of respiratory muscle tone,
- absorption atelectasis with high FiO₂,
- loss of physiological PEEP after intubation,
- supine position,
- diaphragmatic displacement,
- obesity or pregnancy.
Surfactant helps resist collapse, but anaesthesia can overwhelm normal stabilising mechanisms.
Quick check: alveoli and surfactant
Which cells produce surfactant?
Reveal answer
Type II pneumocytes produce surfactant and also help repair injured alveolar epithelium.
How does surfactant stabilise small alveoli?
Reveal answer
As alveoli become smaller, surfactant molecules become more concentrated and reduce surface tension more, preventing small alveoli emptying into larger ones.
Why does general anaesthesia promote atelectasis despite normal surfactant?
Reveal answer
It lowers functional residual capacity, removes physiological PEEP after intubation, encourages dependent collapse, and may cause absorption atelectasis with high inspired oxygen.
EDAIC trap: paediatric airway danger is proportional narrowing. The same millimetre of oedema removes far more radius in a child, so obstruction and desaturation progress quickly.
Paediatric and Special Airway Considerations
Why children obstruct quickly
Children have smaller airways. Because resistance varies with the fourth power of radius, a small amount of oedema or secretions causes a large increase in resistance.
Example:
If airway radius is already small, 1 mm of circumferential oedema produces a much larger proportional narrowing than in an adult.
Clinical relevance:
- croup,
- post-intubation swelling,
- epiglottitis,
- inhalational burns,
- airway infection,
- laryngospasm.
Infant airway features
Important tendencies in infants and young children:
- relatively large tongue,
- more cephalad and anterior larynx,
- floppy, omega-shaped epiglottis,
- small airway diameter,
- high oxygen consumption,
- low oxygen reserve,
- compliant chest wall,
- rapid desaturation during apnoea.
The practical message is that small anatomical differences have major physiological consequences.
Clinical Integration
Why a sedated patient obstructs
Sedation reduces pharyngeal dilator muscle tone. The tongue and soft palate fall posteriorly. Negative inspiratory pressure worsens collapse. Obesity and OSA increase collapsibility.
Treatment:
- reduce sedation if possible,
- head tilt/chin lift/jaw thrust,
- airway adjunct,
- CPAP,
- supraglottic airway or intubation if needed.
Why intubation can cause atelectasis
Intubation bypasses the larynx and prevents expiratory vocal cord adduction. Physiological PEEP is lost. Anaesthesia also reduces FRC and promotes dependent lung collapse. External PEEP helps maintain alveolar recruitment.
Why dry gases are harmful
Dry gases bypassing the upper airway remove heat and water from airway mucosa. Cilia slow, secretions thicken, mucus plugs form, and atelectasis develops. Humidification prevents this.
Why small tubes increase work of breathing
Endotracheal tube resistance rises steeply as radius decreases. A small tube may be acceptable during controlled ventilation but can impose high work during spontaneous breathing or weaning.
Why asthma increases airway resistance
Asthma narrows bronchi and bronchioles through smooth muscle contraction, mucosal oedema, and mucus plugging. Because resistance depends strongly on radius, small narrowing causes large resistance rise. Expiration is especially affected because intrathoracic airway pressure compresses small airways.
Why surfactant deficiency causes respiratory distress
Without surfactant, alveolar surface tension is high. Small alveoli collapse. Lung compliance falls. Work of breathing rises. Fluid is drawn into alveoli. Gas exchange becomes uneven and shunt develops.
Quick check: clinical integration
Why can a small amount of oedema be severe in children?
Reveal answer
Their baseline airway radius is small, so the same absolute swelling causes a much larger proportional narrowing and a steep resistance rise.
What is the common physiology behind sedation obstruction, asthma, and tube narrowing?
Reveal answer
Reduced airway radius increases resistance dramatically; the cause may be soft-tissue collapse, smooth-muscle constriction, oedema, secretions, or the tube itself.
What is the fastest structure-function summary of this module?
Reveal answer
Upper airway protects and conditions; larynx guards the inlet; conducting airways deliver and clear; alveoli exchange gas; surfactant keeps the surface open.
How to use these tables: first separate structure from function, then convert the row into the likely EDAIC consequence: obstruction, aspiration, resistance, dead space, humidity loss, nerve injury, atelectasis, or surfactant failure.
High-Yield Tables
Upper vs lower airway
| Feature | Upper airway | Lower airway |
|---|---|---|
| Structures | Nose, mouth, pharynx | Larynx, trachea, bronchi, bronchioles, alveoli |
| Main roles | Conduct, warm, humidify, filter, protect | Conduct, distribute, clear, exchange gas |
| Main anaesthetic issue | Obstruction and aspiration | Intubation, resistance, bronchospasm, atelectasis |
| Support | Pharynx has no cartilage | Trachea/bronchi have cartilage; bronchioles do not |
Conducting vs respiratory zone
| Feature | Conducting zone | Respiratory zone |
|---|---|---|
| Extent | Trachea to terminal bronchioles | Respiratory bronchioles to alveoli |
| Generations | 0-16 | 17-23 |
| Gas exchange | No | Yes |
| Dead space | Yes | No anatomical dead space |
| Epithelium | Ciliated, mucus-producing proximally | Thin alveolar epithelium |
| Main function | Gas delivery and conditioning | Diffusion of O₂ and CO₂ |
Laryngeal nerve supply
| Nerve | Sensory | Motor |
|---|---|---|
| Internal superior laryngeal | Above cords | None |
| External superior laryngeal | Minimal | Cricothyroid |
| Recurrent laryngeal | Below cords | All intrinsic muscles except cricothyroid |
Surfactant essentials
| Feature | High-yield answer |
|---|---|
| Produced by | Type II pneumocytes |
| Main phospholipid | DPPC |
| Main physical effect | Reduces surface tension |
| Compliance | Increases compliance |
| Work of breathing | Decreases work |
| Small alveoli | Stabilises them |
| Fluid movement | Reduces transudation into alveoli |
| Deficiency | IRDS, atelectasis, low compliance |
| Development | Begins around 24 weeks; matures later |
Definitions and Values to Memorise
| Item | High-yield value or definition | Why it matters |
|---|---|---|
| Conducting zone | Trachea to terminal bronchioles; generations 0-16 | Anatomical dead space, conditioning, resistance, and clearance; no gas exchange. |
| Respiratory zone | Respiratory bronchioles to alveoli; generations 17-23 | Gas exchange begins and becomes dominant. |
| Anatomical dead space | About 150 mL or 2 mL/kg in adults | Increases with artificial airways and affects alveolar ventilation. |
| Water vapour pressure at 37 degrees C | 47 mmHg or 6.3 kPa | Humidification and alveolar gas equation calculations. |
| Laminar resistance | Resistance is proportional to 1/radius^4 | Small airway oedema, bronchospasm, secretions, or small tubes cause large resistance rises. |
| Physiological laryngeal PEEP | About 3-4 cmH2O during expiration | Lost during intubation; external PEEP may be required to maintain FRC. |
| Only vocal cord abductor | Posterior cricoarytenoid | Bilateral recurrent laryngeal nerve injury can critically obstruct the airway. |
| Cricothyroid muscle | External branch of superior laryngeal nerve | Exception to recurrent laryngeal motor supply. |
| Surfactant source | Type II pneumocytes | Also progenitor cells for alveolar epithelial repair. |
| Main surfactant phospholipid | DPPC | Reduces surface tension and improves compliance. |
| Surfactant development | Production begins around 24 weeks; functional maturity later, near 35 weeks | Explains infant respiratory distress syndrome and antenatal corticosteroid use. |
| Laplace law for alveolus | P = 2T/r | Without surfactant, small alveoli require higher pressure and tend to collapse. |
EDAIC Traps
- The pharynx collapses because it is a muscular tube without cartilage.
- Genioglossus is the main pharyngeal dilator.
- Sedation and anaesthesia reduce pharyngeal dilator tone.
- Posterior cricoarytenoid is the only vocal cord abductor.
- Cricothyroid is supplied by the external branch of the superior laryngeal nerve.
- The internal superior laryngeal nerve supplies sensation above the cords.
- The recurrent laryngeal nerve supplies sensation below the cords and motor to all intrinsic laryngeal muscles except cricothyroid.
- Terminal bronchioles are conducting airways; respiratory bronchioles are where gas exchange begins.
- Bronchioles have no cartilage.
- Anatomical dead space is about 150 mL or 2 mL/kg.
- Resistance varies inversely with radius to the fourth power during laminar flow.
- Intubation bypasses humidification and removes physiological laryngeal PEEP.
- Surfactant reduces surface tension, increases compliance, stabilises alveoli, and reduces fluid transudation.
- Do not confuse surfactant-related atelectasis with metabolic causes of hyperthermia; they are separate mechanisms.
- The earliest sign of airway obstruction is often increased work or abnormal airflow, not desaturation.
End-of-Module Summary
The upper airway conducts, warms, humidifies, filters, protects, and participates in speech and swallowing. The nose conditions gas; the pharynx is a collapsible muscular tube; the larynx protects the lower airway and controls airflow through the vocal cords.
The pharynx remains open during wakefulness because dilator muscles such as genioglossus counteract negative inspiratory pressure. Anaesthesia and sedation reduce this tone, making obstruction common. Simple manoeuvres such as jaw thrust, chin lift, airway adjuncts, and CPAP work because they restore structure or pressure to a collapsible airway.
The larynx is anatomically and clinically central. Vocal cords abduct during inspiration and adduct slightly during expiration, creating physiological PEEP. Intubation bypasses this and may promote atelectasis unless external PEEP is used. Laryngeal innervation is high yield: internal superior laryngeal nerve gives sensation above the cords, external superior laryngeal nerve supplies cricothyroid, and recurrent laryngeal nerve supplies sensation below the cords and motor supply to all other intrinsic muscles.
The conducting zone extends from trachea to terminal bronchioles. It conducts, warms, humidifies, filters, and clears gas but does not exchange it. The respiratory zone begins at respiratory bronchioles and is specialised for diffusion. Bronchioles lack cartilage, so smooth muscle tone, lung volume, secretions, and inflammation strongly affect their calibre.
Mucociliary clearance protects the lower airway by moving mucus and trapped particles toward the pharynx. Smoking, dry gases, infection, dehydration, intubation, and anaesthesia impair it.
Surfactant is produced by type II pneumocytes. Its main phospholipid is DPPC. It reduces surface tension, increases compliance, reduces work of breathing, stabilises small alveoli, prevents atelectasis, reduces fluid transudation, and supports innate immunity. Laplace's law explains why surfactant is essential: without it, small alveoli would collapse into larger ones.
Airway structure is airway function. The shape, support, lining, reflexes, and surface tension of the airway determine whether gas reaches the alveoli safely and efficiently.