Lecture note
CO₂ transport, diffusion, and V/Q physiology
Exam Target
Purpose. This module turns CO₂ transport, diffusion, and V/Q matching into a practical diagnostic map for respiratory failure. In EDAIC-style questions, decide whether the problem is CO₂ production, alveolar ventilation, dead space, shunt, V/Q mismatch, diffusion limitation, or altered pulmonary blood flow.
Core idea. CO₂ clearance depends mainly on alveolar ventilation, while oxygenation depends heavily on V/Q matching and shunt. A patient can be hypoxaemic with normal PaCO₂, or hypercapnic because effective alveolar ventilation is too low despite a high respiratory rate.
Revision rule. For every ABG, capnogram, or hypoxaemia stem, ask: is alveolar ventilation low, perfusion absent, ventilation absent, diffusion impaired, or mixed venous oxygen content poor?
Quick check: gas-exchange frame
What is the fastest way to organise a gas-exchange problem?
Reveal answer
Separate ventilation, perfusion, diffusion, shunt, dead space, mixed venous oxygen content, and CO2 production before choosing treatment.
Why can PaCO2 be high despite a high respiratory rate?
Reveal answer
Respiratory rate is not alveolar ventilation. Small tidal volume, high dead space, or severe ventilatory load can make effective alveolar ventilation too low.
What does a low EtCO2 suddenly suggest during anaesthesia?
Reveal answer
Think low pulmonary blood flow, increased dead space, pulmonary embolism, disconnection or leak, airway obstruction, or cardiac arrest, depending on the clinical context.
Carbon Dioxide: The Other Respiratory Gas
Why CO₂ is physiologically powerful
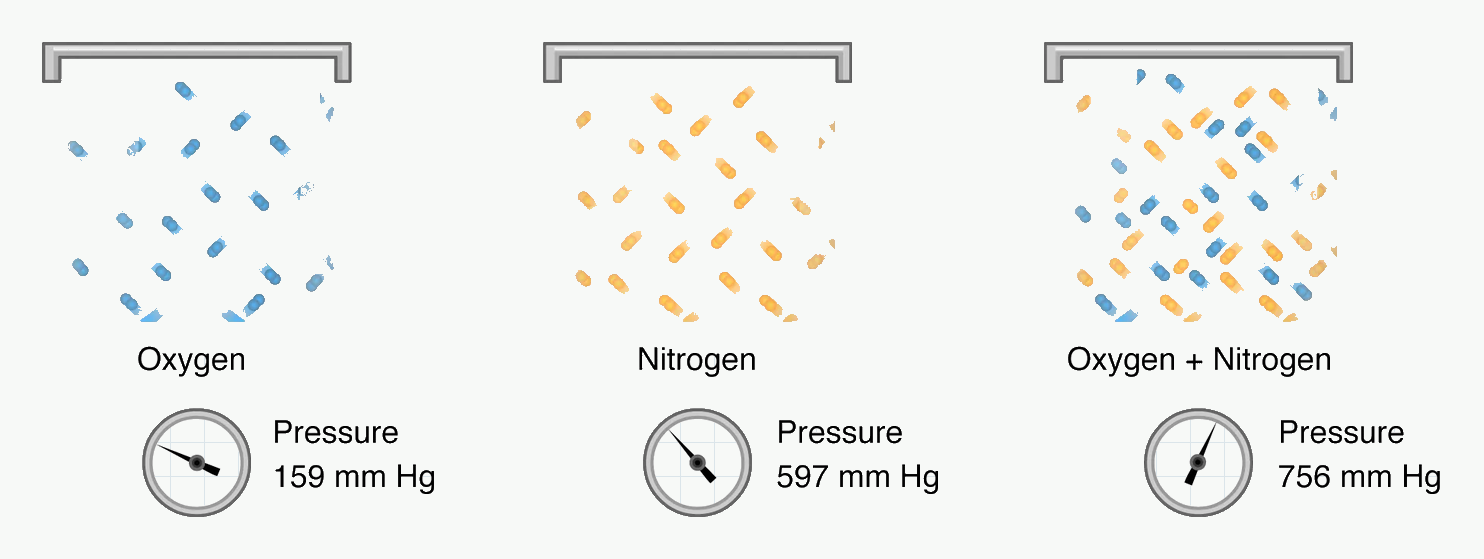
#f7f9f7; diagram labels and line work unchanged. Source link: https://openstax.org/books/anatomy-and-physiology-2e/pages/22-4-gas-exchange.Abbreviations shown: mm Hg = millimetres of mercury.
Start here before V/Q and diffusion: gas transfer is driven by partial pressure gradients, not simply by gas percentages.
For EDAIC, carbon dioxide is not just a waste gas. It is the quickest bedside signal of ventilation, perfusion, metabolism, circuit integrity, and acid-base control.
CO₂ affects:
- acid-base balance,
- cerebral blood flow,
- pulmonary vascular tone,
- ventilatory drive,
- haemoglobin oxygen unloading,
- intracellular pH,
- capnography interpretation,
- anaesthetic depth and emergence,
- arrhythmia risk when severe hypercapnia causes acidosis.
Normal adult CO₂ production, VCO₂, is approximately:
- 200 mL/min at rest,
- often higher with fever, shivering, sepsis, agitation, pain, overfeeding, malignant hyperthermia, or increased work of breathing.
Normal arterial carbon dioxide tension:
- PaCO₂ ≈ 4.7–6.0 kPa, or
- 35–45 mmHg.
The body produces CO₂ continuously. If alveolar ventilation stops, PaCO₂ rises quickly. This is why capnography changes immediately with airway obstruction, apnoea, disconnection, pulmonary embolism, or circulatory collapse.
CO₂ is more soluble than oxygen
CO₂ is far more soluble in blood and tissues than oxygen. Although its molecular weight is only modestly greater than oxygen, its much higher solubility means it diffuses across the alveolar-capillary membrane much more readily.
Clinical consequence:
- Early diffusion disease usually causes hypoxaemia before hypercapnia.
- A patient with pulmonary fibrosis may have low PaO₂ but normal or low PaCO₂ initially because CO₂ diffuses easily and ventilation may increase.
- Hypercapnia usually suggests inadequate alveolar ventilation, severe V/Q abnormality, severe disease, or ventilatory pump failure.
Exam phrase:
CO₂ diffusion is usually not the limiting step; alveolar ventilation is.
Quick check: CO2 as a physiological signal
Why is CO2 not just a waste gas?
Reveal answer
It affects acid-base balance, cerebral blood flow, pulmonary vascular tone, ventilatory drive, haemoglobin oxygen unloading, intracellular pH, and capnography interpretation.
What usually limits CO2 clearance clinically?
Reveal answer
Effective alveolar ventilation. Hypercapnia usually means alveolar ventilation is inadequate, dead space is high, or the disease burden has exceeded ventilatory reserve.
Why does early diffusion disease usually cause hypoxaemia before hypercapnia?
Reveal answer
CO2 is much more soluble than oxygen and usually diffuses more readily across the alveolar-capillary membrane.
Forms of CO₂ Transport in Blood
Overview
CO₂ is carried in blood in three main forms:
How to use this table: first separate measured tension from transport form; then connect the dominant carriage mechanism to acid-base effects.
| Form | Approximate proportion | Main site/form |
|---|---|---|
| Bicarbonate, HCO₃⁻ | ~60–70% | Mainly in plasma after formation in RBCs |
| Carbamino compounds | ~20–30% | Bound to proteins, especially deoxyhaemoglobin |
| Dissolved CO₂ | ~5–10% | Physically dissolved in plasma |
The exact percentages vary between sources and physiological conditions, but the hierarchy is high-yield:
Most CO₂ is transported as bicarbonate.
Dissolved CO₂
Dissolved CO₂ is physically dissolved in plasma.
Although it is a small fraction of total CO₂ carriage, it is crucial because PaCO₂ reflects dissolved CO₂ tension.
Important points:
- Dissolved CO₂ determines PaCO₂.
- PaCO₂ is measured on arterial blood gas analysis.
- PaCO₂ controls ventilatory drive through central chemoreceptors via CSF pH.
- Dissolved CO₂ rapidly crosses the blood-brain barrier.
Clinical relevance:
- A rise in PaCO₂ means dissolved CO₂ has risen.
- This increases carbonic acid formation and lowers pH.
- Hypercapnia causes cerebral vasodilation, which may increase intracranial pressure.
- Hypocapnia causes cerebral vasoconstriction, which may reduce cerebral blood flow.
Bicarbonate transport
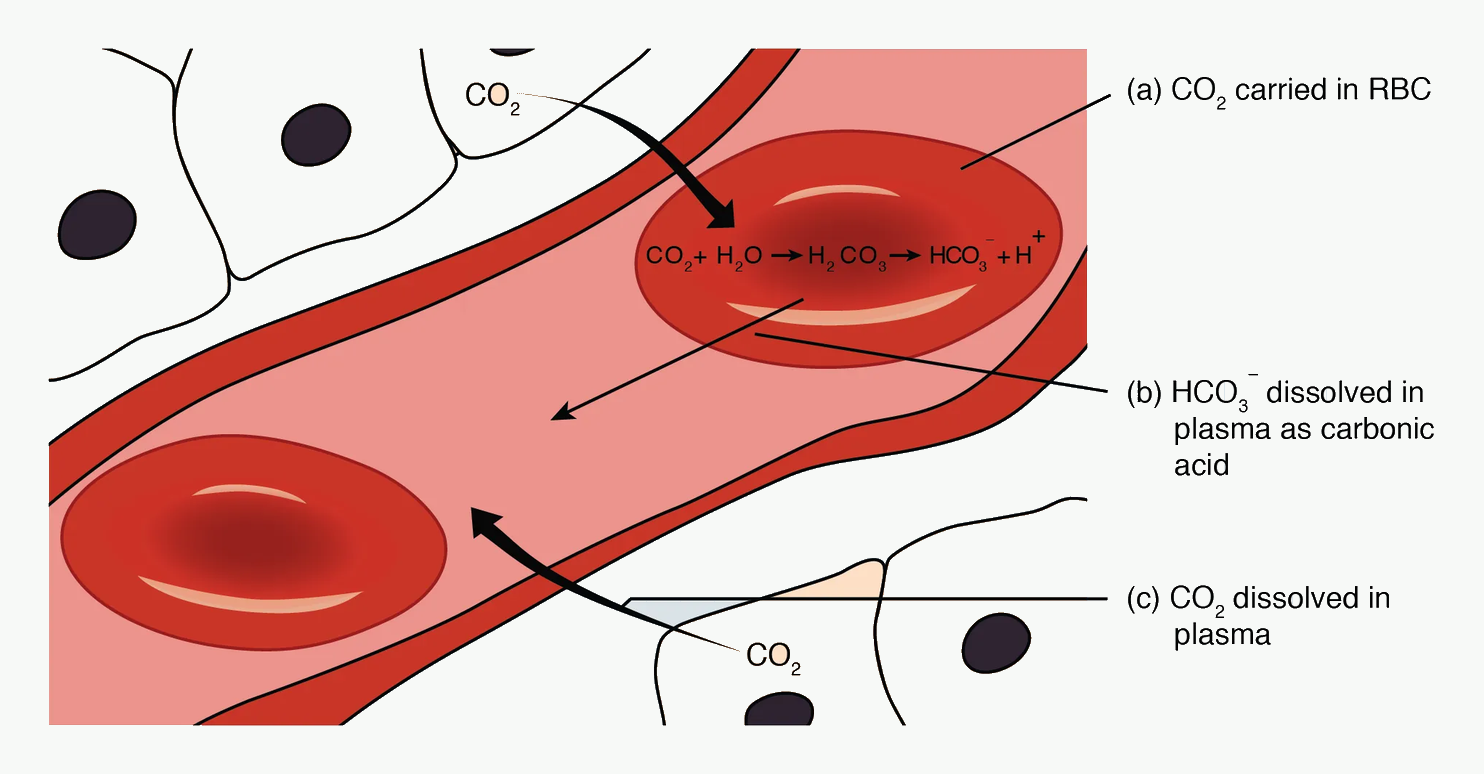
#f7f9f7; diagram labels and line work unchanged. Source link: https://openstax.org/books/anatomy-and-physiology-2e/pages/22-5-transport-of-gases.Abbreviations shown: CO₂ = carbon dioxide; H₂O = water; H₂CO₃ = carbonic acid; HCO₃⁻ = bicarbonate; H⁺ = hydrogen ion; RBC = red blood cell.
Follow the arrows in tissues first: CO2 enters the red cell, carbonic anhydrase makes bicarbonate, chloride shifts inward, and deoxyhaemoglobin buffers H+.
Most CO₂ is converted to bicarbonate in red blood cells.
Step-by-step process in tissues
- CO₂ is produced by tissue metabolism.
- CO₂ diffuses into plasma and then into red blood cells.
- Inside the red cell, carbonic anhydrase rapidly catalyses:
CO₂ + H₂O ⇌ H₂CO₃ ⇌ H⁺ + HCO₃⁻
- Bicarbonate leaves the red cell into plasma.
- Chloride enters the red cell to maintain electrical neutrality.
- Hydrogen ions are buffered mainly by deoxyhaemoglobin.
This is efficient because red blood cells contain abundant carbonic anhydrase, whereas plasma contains very little.
Chloride shift
The chloride shift, also called the Hamburger effect, is the movement of bicarbonate out of red blood cells in exchange for chloride entering the red blood cell.
Mechanism:
- CO₂ is converted to HCO₃⁻ inside the red cell.
- HCO₃⁻ concentration rises in the red cell.
- HCO₃⁻ leaves the red cell via a Cl⁻/HCO₃⁻ exchanger.
- Cl⁻ enters to maintain electroneutrality.
Purpose:
- prevents bicarbonate accumulation inside the red cell,
- allows continued CO₂ conversion to bicarbonate,
- increases total CO₂ carriage,
- helps maintain electrical neutrality.
Exam trap:
The chloride shift occurs mainly in systemic tissues during CO₂ loading; it reverses in the lungs during CO₂ unloading.
Haemoglobin buffering of H⁺
When CO₂ is converted to bicarbonate, H⁺ is produced. If H⁺ accumulated freely, red cell pH would fall and the reaction would slow.
Haemoglobin buffers H⁺, especially deoxyhaemoglobin.
Why deoxyhaemoglobin matters:
- It is a better proton buffer than oxyhaemoglobin.
- It accepts H⁺ more readily.
- This promotes continued bicarbonate formation.
Clinical link:
In tissues, oxygen is unloaded and haemoglobin becomes deoxygenated. This makes haemoglobin better able to carry CO₂. This is part of the Haldane effect.
Carbamino compounds
CO₂ can bind directly to terminal amino groups of proteins, especially globin chains of haemoglobin.
This forms carbaminohaemoglobin.
Important points:
- CO₂ binds to the protein part of haemoglobin, not the haem iron.
- Deoxyhaemoglobin forms carbamino compounds more readily than oxyhaemoglobin.
- Carbamino carriage accounts for roughly 20–30% of CO₂ transport.
Do not confuse:
- Carbaminohaemoglobin = CO₂ bound to globin chains.
- Carboxyhaemoglobin = carbon monoxide bound to haem iron.
- Oxyhaemoglobin = oxygen bound to haem iron.
- Methaemoglobin = ferric Fe³⁺ haemoglobin.
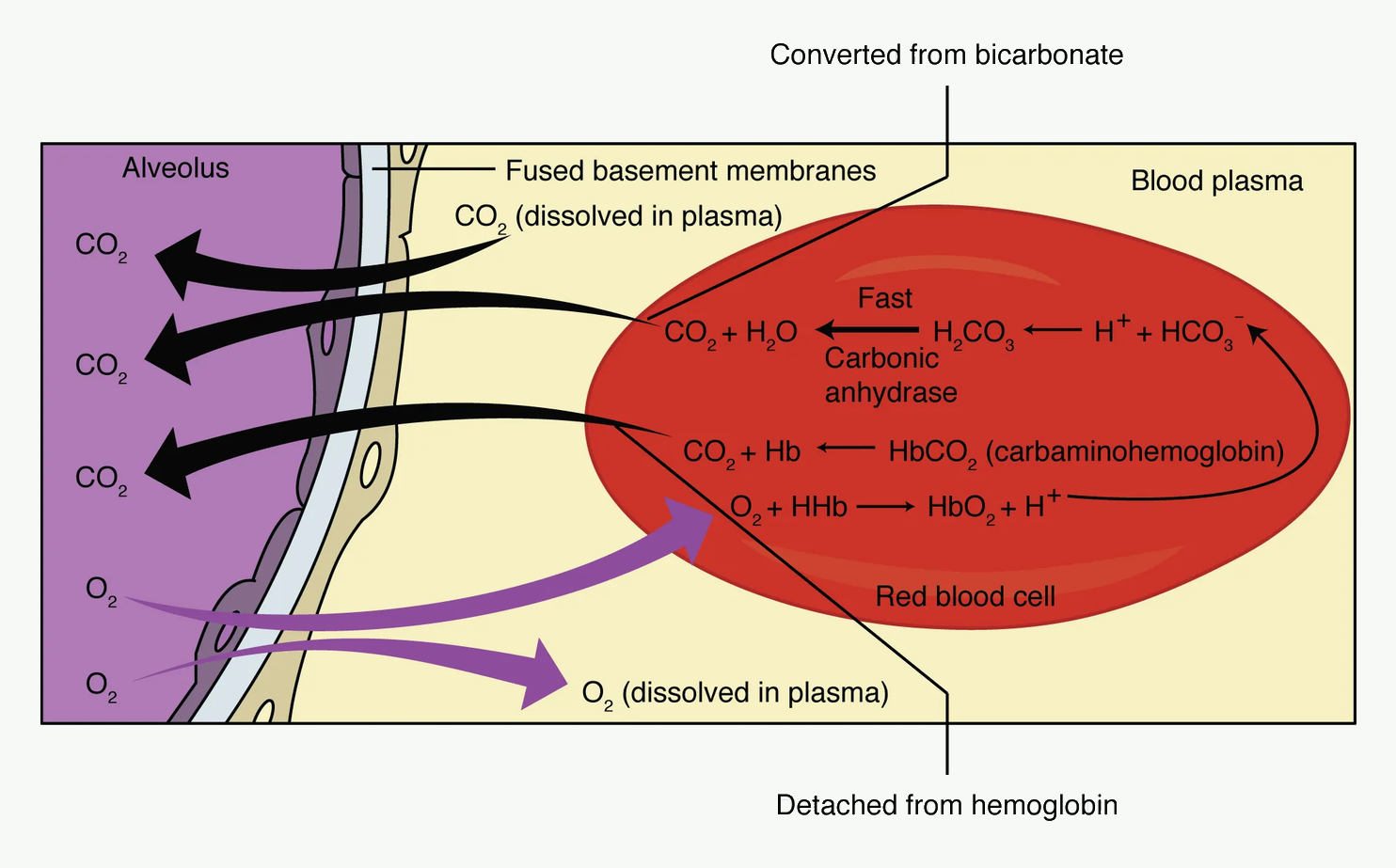
What happens in the lungs?
#f7f9f7; diagram labels and line work unchanged. Source link: https://openstax.org/books/anatomy-and-physiology-2e/pages/22-4-gas-exchange.Abbreviations shown: CO₂ = carbon dioxide; O₂ = oxygen; H₂O = water; H₂CO₃ = carbonic acid; HCO₃⁻ = bicarbonate; H⁺ = hydrogen ion; Hb = haemoglobin; HbO₂ = oxyhaemoglobin; HHb = deoxyhaemoglobin.
Use this as the tissue half of the Haldane effect: oxygen unloading creates deoxyhaemoglobin, which improves CO2 carriage and H+ buffering.
In pulmonary capillaries, the process reverses.
- Oxygen enters red blood cells and binds haemoglobin.
- Oxygenation of haemoglobin reduces its ability to buffer H⁺ and carry CO₂.
- H⁺ is released and combines with HCO₃⁻.
- Bicarbonate re-enters red cells in exchange for chloride moving out.
- Carbonic anhydrase converts H⁺ + HCO₃⁻ back to CO₂ + H₂O.
- CO₂ diffuses into alveoli and is exhaled.
This is why oxygenation in the lung promotes CO₂ unloading.
Quick check: CO2 carriage
What are the three main forms of CO2 transport?
Reveal answer
Mostly bicarbonate, with smaller amounts as carbamino compounds and dissolved CO2.
Why does dissolved CO2 matter if it is only a small fraction?
Reveal answer
Dissolved CO2 determines PaCO2, crosses the blood-brain barrier, and drives CSF pH and central ventilatory response.
What is the chloride shift?
Reveal answer
Bicarbonate leaves the red cell in exchange for chloride during tissue CO2 loading; the process reverses in the lungs.
Haldane Effect, Bohr Effect, and CO₂ Dissociation Curve
Haldane effect
The Haldane effect describes the fact that deoxygenated haemoglobin carries more CO₂ than oxygenated haemoglobin.
A good exam definition:
The Haldane effect is the increased ability of deoxygenated haemoglobin to carry CO₂ and buffer H⁺ compared with oxygenated haemoglobin.
It occurs because deoxyhaemoglobin:
- forms carbamino compounds more readily,
- buffers H⁺ more effectively, allowing more bicarbonate formation.
Physiological importance
In tissues:
- oxygen leaves haemoglobin,
- haemoglobin becomes deoxygenated,
- CO₂ carriage improves.
In lungs:
- oxygen binds haemoglobin,
- haemoglobin becomes oxygenated,
- CO₂ carriage falls,
- CO₂ is released into alveoli.
The Haldane effect therefore helps CO₂ loading in tissues and CO₂ unloading in lungs.
Bohr effect versus Haldane effect
These two effects are commonly confused.
| Effect | What changes? | Main consequence |
|---|---|---|
| Bohr effect | CO₂/H⁺ affect O₂ binding | Increased CO₂/H⁺ shifts HbO₂ curve right and promotes O₂ unloading |
| Haldane effect | O₂ binding affects CO₂ carriage | Deoxygenated Hb carries more CO₂; oxygenation promotes CO₂ unloading |
Memory aid:
- Bohr: CO₂ helps unload O₂.
- Haldane: O₂ status affects CO₂ carriage.
CO₂ dissociation curve
The CO₂ dissociation curve relates CO₂ content of blood to PCO₂.
Compared with the O₂ dissociation curve, the CO₂ curve is:
- more linear over the physiological range,
- steeper within normal PCO₂ range,
- without a clear plateau,
- shifted by oxygenation status.
Deoxygenated blood carries more CO₂ at any given PCO₂ than oxygenated blood. This is the Haldane effect shown graphically.
Clinical implication:
Oxygenation of blood in pulmonary capillaries shifts the CO₂ curve downward, helping CO₂ leave the blood for exhalation.
PaCO₂ and alveolar ventilation
PaCO₂ is determined mainly by the balance between CO₂ production and alveolar ventilation.
Simplified relationship:
PaCO₂ ∝ VCO₂ / VA
where:
- VCO₂ = CO₂ production,
- VA = alveolar ventilation.
If CO₂ production increases and ventilation does not increase, PaCO₂ rises.
If alveolar ventilation decreases and CO₂ production is unchanged, PaCO₂ rises.
If ventilation increases relative to CO₂ production, PaCO₂ falls.
Alveolar ventilation equation
A useful clinical expression is:
PaCO₂ = K × VCO₂ / VA
The constant depends on units. The concept is more important than the exact constant:
PaCO₂ rises when CO₂ production increases or alveolar ventilation decreases.
Alveolar ventilation is:
VA = respiratory rate × (tidal volume − dead space)
This means a patient can have a high respiratory rate but poor CO₂ clearance if tidal volume is small and most ventilation is dead space.
Clinical examples:
- rapid shallow breathing in respiratory failure,
- severe COPD with high dead space,
- small tidal volumes without adequate respiratory rate,
- circuit dead space added by equipment,
- pulmonary embolism increasing alveolar dead space.
Causes of hypercapnia
Hypercapnia is usually caused by inadequate alveolar ventilation relative to CO₂ production.
Causes include:
| Mechanism | Examples |
|---|---|
| Reduced respiratory drive | Opioids, sedatives, brainstem injury |
| Neuromuscular weakness | Myasthenia, Guillain–Barré, residual blockade |
| Increased load | COPD, severe asthma, obesity, chest wall disease |
| Increased dead space | Pulmonary embolism, emphysema, low cardiac output |
| Increased CO₂ production | Fever, shivering, sepsis, malignant hyperthermia |
| Inadequate ventilator settings | Low minute ventilation, high apparatus dead space |
Clinical note:
A sudden fall in end-tidal CO₂ may mean reduced CO₂ production, increased alveolar dead space, low pulmonary blood flow, disconnection, airway obstruction, or cardiac arrest. A sudden rise may mean hypoventilation, increased CO₂ production, rebreathing, or return of circulation after arrest.
Quick check: Haldane and Bohr
What is the Haldane effect?
Reveal answer
Deoxygenated haemoglobin carries more CO2 and buffers H+ better than oxygenated haemoglobin.
How is the Bohr effect different?
Reveal answer
The Bohr effect is CO2 and H+ shifting haemoglobin oxygen affinity; the Haldane effect is oxygenation status changing CO2 carriage.
What relationship links PaCO2 with ventilation?
Reveal answer
PaCO2 is proportional to CO2 production divided by alveolar ventilation. Alveolar ventilation equals respiratory rate times tidal volume minus dead space.
Alveolar Diffusion
Definition
Diffusion is the passive movement of molecules from a region of higher partial pressure to a region of lower partial pressure.
In the lung, diffusion refers to gas transfer across the alveolar-capillary membrane:
- oxygen diffuses from alveolar gas into pulmonary capillary blood,
- carbon dioxide diffuses from pulmonary capillary blood into alveolar gas.
Fick's law of diffusion
For a gas crossing a membrane:
Rate of diffusion ∝ (Area × diffusion coefficient × pressure gradient) / thickness
The diffusion coefficient depends on:
- gas solubility,
- molecular weight.
More formally:
Diffusion coefficient ∝ solubility / √molecular weight
Therefore diffusion is faster when:
- surface area is large,
- membrane is thin,
- partial pressure gradient is large,
- gas is highly soluble,
- molecular weight is low.
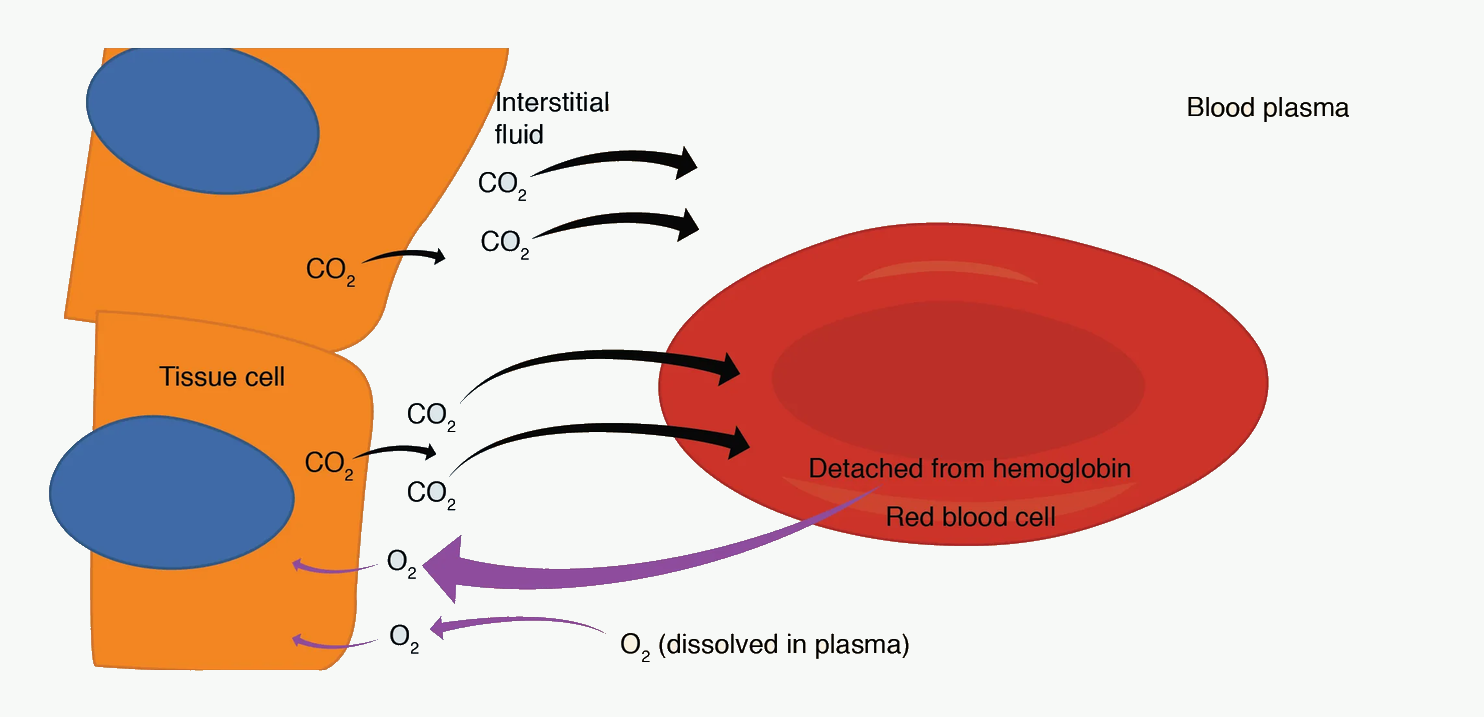
The alveolar-capillary membrane
#f7f9f7; diagram labels and line work unchanged. Source link: https://openstax.org/books/anatomy-and-physiology-2e/pages/22-4-gas-exchange.Abbreviations shown: CO₂ = carbon dioxide; O₂ = oxygen; H₂O = water; H₂CO₃ = carbonic acid; HCO₃⁻ = bicarbonate; H⁺ = hydrogen ion; Hb = haemoglobin; HbO₂ = oxyhaemoglobin; HHb = deoxyhaemoglobin.
Pair this with the tissue figure. In the lung, oxygenation of haemoglobin promotes CO2 unloading, while diffusion depends on surface area, thickness, solubility, and gradient.
The diffusion pathway includes:
- alveolar gas,
- surfactant layer,
- type I pneumocyte,
- epithelial basement membrane,
- interstitial space,
- capillary basement membrane,
- capillary endothelium,
- plasma,
- red cell membrane,
- cytoplasm,
- haemoglobin binding site.
The healthy membrane is extremely thin, approximately 0.5–1.0 micrometre, and has a large surface area.
Normal red blood cell transit time through pulmonary capillaries at rest is approximately 0.75 seconds.
Oxygen equilibration usually completes in about 0.25–0.3 seconds under normal conditions, leaving a large safety margin. CO₂ equilibration is even faster.
Why CO₂ diffuses faster than O₂
CO₂ has a higher molecular weight than O₂, but it is far more soluble. Solubility dominates, so CO₂ diffuses much faster through biological membranes.
Clinical consequence:
- Diffusion impairment tends to reduce oxygen transfer before CO₂ transfer.
- Hypercapnia in lung disease usually means severe disease, high dead space, ventilatory failure, or inability to increase minute ventilation.
Perfusion-limited versus diffusion-limited gases
Perfusion-limited transfer
A gas is perfusion-limited when it equilibrates rapidly between alveolar gas and capillary blood. Transfer then depends mainly on blood flow.
Examples:
- nitrous oxide,
- oxygen under normal resting conditions.
For perfusion-limited gases, increasing pulmonary blood flow increases gas transfer.
Diffusion-limited transfer
A gas is diffusion-limited when it does not fully equilibrate by the time blood leaves the pulmonary capillary. Transfer depends mainly on membrane properties and gradient.
Examples:
- carbon monoxide,
- oxygen in severe diffusion disease, exercise at altitude, or thickened membrane states.
Carbon monoxide is diffusion-limited because it binds avidly to haemoglobin, keeping capillary partial pressure of CO very low, so the gradient persists throughout capillary transit.
DLCO: diffusing capacity for carbon monoxide
Diffusing capacity of the lung for carbon monoxide, DLCO, is used clinically to assess gas transfer.
Why carbon monoxide is used:
- it binds strongly to haemoglobin,
- capillary PCO remains extremely low,
- uptake reflects diffusion capacity of the alveolar-capillary membrane and pulmonary capillary blood volume.
DLCO is reduced in:
- pulmonary fibrosis,
- emphysema,
- pulmonary vascular disease,
- anaemia,
- pulmonary oedema,
- after lung resection.
DLCO may be increased in:
- pulmonary haemorrhage,
- polycythaemia,
- increased pulmonary blood volume.
Important correction:
Anaemia lowers DLCO because less haemoglobin is available to bind CO. DLCO interpretation should consider haemoglobin concentration.
Causes of diffusion impairment
Diffusion is impaired by:
| Fick factor | Disease example |
|---|---|
| Reduced surface area | Emphysema, lung resection |
| Increased thickness | Pulmonary fibrosis, pulmonary oedema, ARDS |
| Reduced gradient | Low alveolar oxygen, altitude |
| Reduced capillary blood volume | Pulmonary vascular disease, embolism |
| Shortened transit time | Exercise in severe disease |
Clinical feature:
Diffusion impairment often worsens during exercise because capillary transit time shortens and oxygen has less time to equilibrate.
Diffusion and anaesthesia
General anaesthesia can worsen gas exchange by:
- reducing FRC,
- causing atelectasis,
- increasing shunt,
- impairing hypoxic pulmonary vasoconstriction,
- reducing respiratory muscle tone,
- using high FiO₂ and causing absorption atelectasis,
- positive pressure ventilation altering regional ventilation and perfusion.
Pure diffusion limitation is less common than V/Q mismatch and shunt in routine anaesthesia, but diffusion principles explain why oedema, fibrosis, ARDS, and emphysema impair oxygenation.
Quick check: diffusion
Which factors in Fick's law improve diffusion?
Reveal answer
Greater surface area, greater diffusion coefficient, and a larger partial-pressure gradient improve diffusion; thicker membrane worsens it.
What is the difference between perfusion-limited and diffusion-limited transfer?
Reveal answer
Perfusion-limited transfer is limited by blood flow after rapid equilibration. Diffusion-limited transfer is limited by membrane transfer and may not equilibrate before blood leaves the capillary.
Why is carbon monoxide used to measure diffusing capacity?
Reveal answer
Carbon monoxide binds haemoglobin avidly, keeping capillary partial pressure very low, so uptake reflects membrane and capillary transfer capacity.
Ventilation-Perfusion Ratio
Definition
The ventilation-perfusion ratio, V/Q, compares alveolar ventilation to pulmonary blood flow for a lung unit.
V/Q = alveolar ventilation / pulmonary perfusion
Whole-lung average values at rest:
- alveolar ventilation ≈ 4 L/min,
- pulmonary blood flow ≈ 5 L/min,
- average V/Q ≈ 0.8.
This average hides large regional differences.
Why V/Q matching matters
For efficient gas exchange, alveoli must receive both:
- ventilation, to bring O₂ and remove CO₂,
- perfusion, to deliver venous blood and remove oxygenated blood.
A perfectly ventilated alveolus with no blood flow cannot oxygenate blood. A perfectly perfused alveolus with no ventilation cannot oxygenate blood either.
Clinical concept:
Gas exchange is a matching problem, not only an oxygen concentration problem.
V/Q extremes
Shunt: V/Q = 0
A shunt unit is perfused but not ventilated.
- Ventilation = 0.
- Perfusion persists.
- V/Q = 0.
- Blood leaves the unit with venous gas tensions.
Examples:
- atelectasis,
- pneumonia consolidation,
- pulmonary oedema-filled alveoli,
- ARDS collapsed/flooded units,
- right-to-left intracardiac shunt.
Dead space: V/Q = infinity
A dead-space unit is ventilated but not perfused.
- Ventilation persists.
- Perfusion = 0.
- V/Q approaches infinity.
- Alveolar gas resembles inspired gas.
Examples:
- pulmonary embolism,
- low cardiac output reducing pulmonary perfusion,
- overdistended alveoli from excessive PEEP,
- emphysematous destruction of capillary bed.
Low V/Q and high V/Q
Most clinical problems are not perfect shunt or perfect dead space. They are regions of low or high V/Q.
How to use this table: read each row as ventilation relative to perfusion, then predict oxygen response and CO2 clearance.
| V/Q state | Meaning | Gas pattern |
|---|---|---|
| Low V/Q | Perfusion exceeds ventilation | Low PAO₂, high PACO₂; hypoxaemia |
| Normal V/Q | Matched ventilation and perfusion | Efficient exchange |
| High V/Q | Ventilation exceeds perfusion | High PAO₂, low PACO₂; wasted ventilation |
| Shunt | Perfusion with no ventilation | Venous admixture |
| Dead space | Ventilation with no perfusion | Wasted ventilation |
Low V/Q causes hypoxaemia because blood leaving poorly ventilated units has low oxygen content. High V/Q causes wasted ventilation because ventilation is delivered to regions with too little blood flow.
V/Q mismatch and supplemental oxygen
V/Q mismatch usually improves with supplemental oxygen because poorly ventilated alveoli still receive some ventilation. Increasing FiO₂ raises alveolar PO₂ in those units and improves oxygenation.
True shunt responds poorly because the shunted blood never sees alveolar gas.
Exam phrase:
Oxygen improves low V/Q more than true shunt.
Why CO₂ is often normal in V/Q mismatch
V/Q mismatch commonly causes hypoxaemia before hypercapnia.
Reasons:
- CO₂ diffuses more readily than O₂.
- CO₂ dissociation curve is more linear.
- Increased ventilation of better lung units can compensate for CO₂ elimination.
- Central chemoreceptors increase ventilation if PaCO₂ rises.
But severe disease, fatigue, increased dead space, respiratory depression, or COPD can cause hypercapnia.
Quick check: V/Q extremes
What is the approximate average whole-lung V/Q ratio?
Reveal answer
About 0.8, because total alveolar ventilation is normally slightly less than pulmonary blood flow.
What are the two extremes of V/Q?
Reveal answer
Shunt is perfusion without ventilation, where V/Q equals zero. Dead space is ventilation without effective perfusion, where V/Q approaches infinity.
Why does oxygen help V/Q mismatch better than true shunt?
Reveal answer
Low V/Q units still receive some ventilation, so higher alveolar oxygen can improve capillary oxygenation. True shunt blood bypasses ventilated gas and remains poorly oxygenated.
Regional V/Q Variation in the Upright Lung
Gravity affects both ventilation and perfusion
In an upright person, both ventilation and perfusion increase from apex to base.
However, perfusion increases more steeply than ventilation.
Therefore:
- V/Q is higher at the apex,
- V/Q is lower at the base.
Approximate values:
| Region | Ventilation | Perfusion | V/Q |
|---|---|---|---|
| Apex | Low | Very low | High, around 3 |
| Middle | Moderate | Moderate | Around 1 |
| Base | High | Very high | Low, around 0.6 |
Apex gas composition
At the apex:
- ventilation is relatively greater than perfusion,
- V/Q is high,
- PAO₂ is high,
- PACO₂ is low,
- blood flow is low.
Apex resembles a mild dead-space pattern.
Base gas composition
At the base:
- perfusion is relatively greater than ventilation,
- V/Q is low,
- PAO₂ is lower,
- PACO₂ is higher,
- blood flow is high.
Base resembles a mild shunt-like pattern.
Why whole-lung V/Q mismatch exists normally
Even in health, V/Q is not uniform. This contributes to the normal alveolar-arterial oxygen gradient.
Small physiological venous admixture also occurs from:
- bronchial venous drainage,
- Thebesian veins draining into the left heart,
- minor regional V/Q inequality.
This is why PaO₂ is normally slightly lower than PAO₂.
Supine, lateral, and anaesthetised patients
Body position changes regional ventilation and perfusion.
Supine position
Gravity creates a dorsal-ventral gradient. Dependent posterior lung regions receive more perfusion, but anaesthesia often causes dependent atelectasis. This creates low V/Q and shunt.
Lateral position
In the awake lateral patient:
- dependent lung receives more perfusion,
- dependent diaphragm may ventilate well,
- matching can be relatively good.
Under anaesthesia and paralysis:
- dependent lung receives more perfusion,
- non-dependent lung may receive more ventilation,
- dependent lung may collapse,
- V/Q mismatch increases.
This is central to one-lung ventilation.
Quick check: regional V/Q
Which region has the highest V/Q ratio in an upright lung?
Reveal answer
The apex, because perfusion falls more than ventilation as height increases above the heart.
Why is the base lower V/Q despite better ventilation?
Reveal answer
Both ventilation and perfusion increase toward the base, but perfusion increases more steeply, so the ratio falls.
Why does anaesthesia worsen dependent V/Q mismatch?
Reveal answer
Anaesthesia reduces FRC and promotes dependent airway closure and atelectasis, while perfusion often remains greatest in dependent regions.
West Lung Zones
The pressure relationships
West zones describe how alveolar pressure, arterial pressure, and venous pressure determine pulmonary blood flow.
Key pressures:
- PA = alveolar pressure,
- Pa = pulmonary arterial pressure,
- Pv = pulmonary venous pressure.
Do not confuse:
- PA = alveolar pressure in West zones,
- PaO₂ = arterial oxygen tension.
Zone 1
Pressure relationship:
PA > Pa > Pv
Alveolar pressure exceeds pulmonary arterial pressure, so capillaries are compressed and flow is absent or minimal.
Zone 1 is alveolar dead space.
Normally, zone 1 is absent or very small in healthy lungs at rest.
It increases with:
- hypovolaemia,
- low pulmonary arterial pressure,
- high alveolar pressure,
- excessive PEEP,
- positive pressure ventilation,
- pulmonary embolism-like physiology,
- low cardiac output.
Clinical consequence:
- increased dead space,
- wasted ventilation,
- increased PaCO₂ if ventilation cannot compensate,
- larger PaCO₂-EtCO₂ gradient.
Zone 2
Pressure relationship:
Pa > PA > Pv
Pulmonary arterial pressure exceeds alveolar pressure, but alveolar pressure exceeds venous pressure.
Flow depends on:
Pa − PA
not on Pa − Pv.
This is sometimes called the waterfall effect or Starling resistor effect.
As pulmonary arterial pressure rises down the lung, flow increases.
Zone 3
Pressure relationship:
Pa > Pv > PA
Both arterial and venous pressures exceed alveolar pressure, so capillaries remain open and flow is continuous.
Flow depends on:
Pa − Pv
Zone 3 has the greatest blood flow and is found in dependent lung regions under normal conditions.
Zone 4 — low-volume zone
Some descriptions include zone 4 at very low lung volumes.
Mechanism:
- extra-alveolar vessels narrow because lung volume is low,
- interstitial pressure and reduced radial traction compress small vessels,
- blood flow falls in the most dependent lung despite high vascular pressure.
Seen with:
- very low lung volumes,
- dependent atelectasis,
- pulmonary oedema,
- reduced FRC.
Exam priority:
West zones 1-3 are the core EDAIC knowledge. Zone 4 is useful clinically but less central.
West zones during anaesthesia and ventilation
Positive pressure ventilation and PEEP increase alveolar pressure. This can:
- increase zone 1 conditions,
- reduce perfusion to overdistended alveoli,
- increase alveolar dead space,
- increase pulmonary vascular resistance if excessive,
- improve oxygenation by recruiting collapsed alveoli if appropriately applied.
Therefore PEEP has two opposite effects:
| Helpful effect | Harmful effect |
|---|---|
| Recruits collapsed alveoli and reduces shunt | Overdistends alveoli and increases dead space |
| Improves V/Q in dependent lung | Reduces venous return and cardiac output if excessive |
| Improves oxygenation in atelectasis/ARDS | May increase pulmonary vascular resistance |
The clinical skill is finding the balance.
Quick check: West zones
What pressure relationship defines West zone 1?
Reveal answer
Alveolar pressure exceeds arterial and venous pressure, so perfusion is absent or very low and alveolar dead space increases.
What pressure relationship defines West zone 2?
Reveal answer
Arterial pressure exceeds alveolar pressure, which exceeds venous pressure. Flow depends mainly on arterial pressure minus alveolar pressure.
How can PEEP affect West zones?
Reveal answer
PEEP can recruit collapsed lung and improve oxygenation, but excessive PEEP can raise alveolar pressure, compress capillaries, and increase dead space.
Hypoxaemia: Mechanisms and Oxygen Response
The five classic mechanisms
Hypoxaemia can be caused by:
- low inspired oxygen tension,
- alveolar hypoventilation,
- diffusion impairment,
- V/Q mismatch,
- right-to-left shunt.
A sixth related issue is reduced mixed venous oxygen content, which can worsen arterial oxygenation in shunt or V/Q mismatch.
Low inspired oxygen tension
Mechanism:
- low barometric pressure or low FiO₂ lowers PIO₂,
- alveolar oxygen falls,
- arterial oxygen falls.
Examples:
- altitude,
- incorrect gas mixture,
- oxygen supply failure,
- breathing hypoxic gas.
A-a gradient:
- normal.
Response to oxygen:
- improves if FiO₂ is increased and the delivery system works.
Alveolar hypoventilation
Mechanism:
- alveolar ventilation falls,
- PaCO₂ rises,
- alveolar gas equation shows PAO₂ falls,
- PaO₂ falls.
Examples:
- opioids,
- sedatives,
- residual neuromuscular blockade,
- CNS depression,
- severe obesity hypoventilation,
- neuromuscular weakness,
- inadequate ventilator minute ventilation.
A-a gradient:
- usually normal if lungs are otherwise normal.
Response to oxygen:
- PaO₂ improves with oxygen,
- but PaCO₂ remains high unless ventilation improves.
Clinical warning:
Oxygen can correct SpO₂ while hypercapnia worsens. Ventilation must be addressed.
Diffusion impairment
Mechanism:
- gas transfer across alveolar-capillary membrane is slowed,
- oxygen may not fully equilibrate before blood leaves the capillary,
- worsens during exercise or low alveolar oxygen.
Examples:
- pulmonary fibrosis,
- pulmonary oedema,
- ARDS,
- severe emphysema with reduced surface area.
A-a gradient:
- increased.
Response to oxygen:
- usually improves because increased alveolar PO₂ increases the diffusion gradient.
V/Q mismatch
Mechanism:
- some lung units receive too little ventilation for their perfusion,
- blood leaving those units has low oxygen content,
- high V/Q units cannot fully compensate because haemoglobin is already near saturated.
Examples:
- asthma,
- COPD,
- pneumonia,
- pulmonary oedema,
- atelectasis,
- pulmonary embolism with secondary redistribution,
- anaesthesia-induced dependent collapse.
A-a gradient:
- increased.
Response to oxygen:
- usually improves, often substantially.
Why high V/Q cannot compensate for low V/Q:
High V/Q units can raise PaO₂ and dissolved oxygen, but haemoglobin is already nearly fully saturated. They cannot add enough extra oxygen content to compensate for poorly oxygenated blood from low V/Q units.
Right-to-left shunt
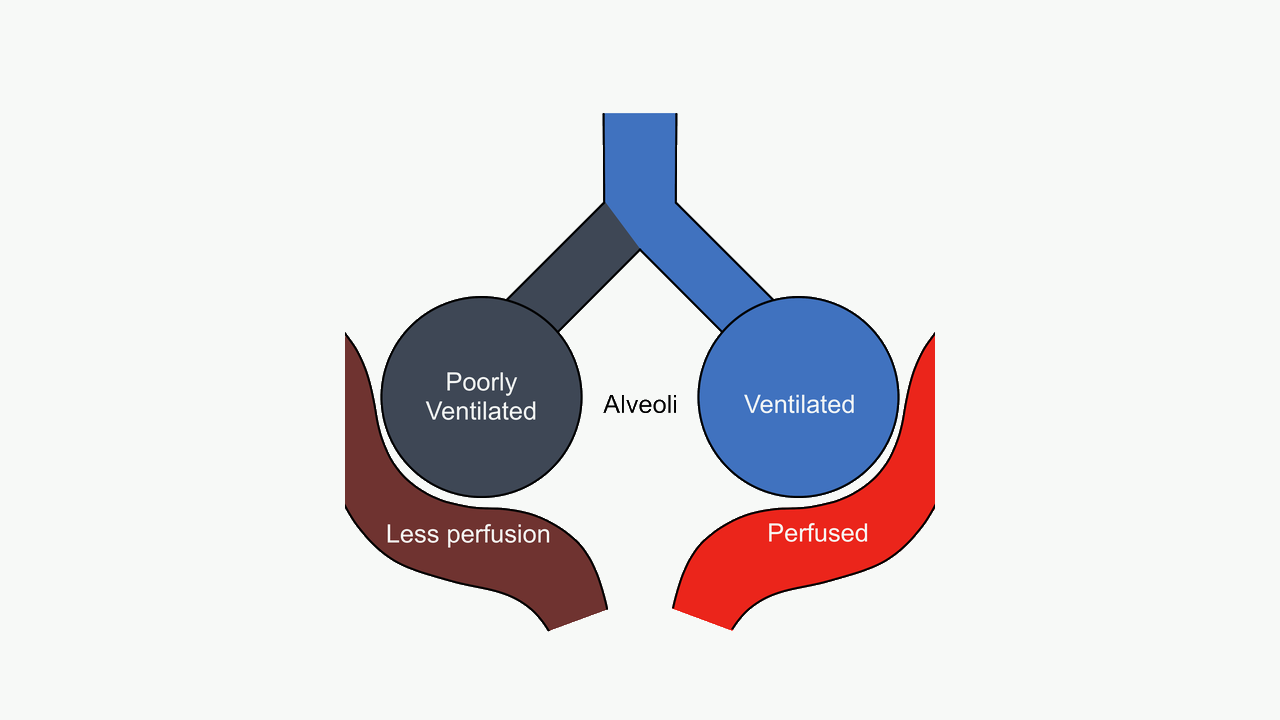
#f7f9f7; diagram labels and line work unchanged. Source link: https://commons.wikimedia.org/wiki/File:Pulmonary_shunt_diagram.png.Use this as the V/Q = 0 extreme: blood reaches unventilated lung units and therefore responds poorly to oxygen until alveoli are recruited or the cause is treated.
Mechanism:
- blood reaches arterial circulation without contacting ventilated alveoli,
- shunted venous blood mixes with oxygenated blood,
- arterial oxygen content falls.
Types:
| Type | Examples |
|---|---|
| Anatomical shunt | Intracardiac right-to-left shunt, pulmonary AV malformation |
| Physiological/intrapulmonary shunt | Atelectasis, consolidation, ARDS, flooded alveoli |
| Normal small shunt | Bronchial veins, Thebesian veins |
A-a gradient:
- increased.
Response to oxygen:
- poor in true shunt,
- because shunted blood never sees alveolar oxygen.
Clinical examples:
- lobar collapse,
- severe pneumonia,
- ARDS,
- one-lung ventilation,
- congenital cyanotic heart disease.
Comparing mechanisms of hypoxaemia
How to use this table: pair A-a gradient with oxygen response; that combination identifies the mechanism faster than memorising disease names.
| Cause | PaCO₂ | A-a gradient | Response to O₂ |
|---|---|---|---|
| Low FiO₂/altitude | Normal/low | Normal | Good |
| Hypoventilation | High | Normal | Good for PaO₂; ventilation still needed |
| Diffusion impairment | Normal/low initially | Increased | Good |
| V/Q mismatch | Normal/low or high if severe | Increased | Good/moderate |
| Shunt | Normal/low or high if severe | Increased | Poor |
Quick check: hypoxaemia mechanisms
Which mechanisms usually have a normal A-a gradient?
Reveal answer
Low inspired oxygen and pure hypoventilation usually have a normal A-a gradient because the alveolar-capillary unit can still equilibrate.
Which mechanisms usually widen the A-a gradient?
Reveal answer
Diffusion impairment, V/Q mismatch, and shunt widen the A-a gradient.
Why does true shunt respond poorly to oxygen?
Reveal answer
The shunted blood does not contact ventilated alveoli, so increasing inspired oxygen mainly affects already ventilated units and has limited effect on mixed arterial content.
Shunt Physiology in Depth
Venous admixture
Venous admixture is the mixing of deoxygenated or poorly oxygenated blood with oxygenated pulmonary venous blood, reducing arterial oxygen content.
Sources:
- true anatomical shunt,
- perfusion of non-ventilated alveoli,
- severe low V/Q regions,
- bronchial and Thebesian venous drainage.
Shunt equation
The classical shunt fraction equation is:
Qs/Qt = (CcO₂ − CaO₂) / (CcO₂ − CvO₂)
where:
- Qs = shunt blood flow,
- Qt = total pulmonary blood flow/cardiac output,
- CcO₂ = ideal end-capillary oxygen content,
- CaO₂ = arterial oxygen content,
- CvO₂ = mixed venous oxygen content.
Clinical meaning:
- It estimates the fraction of cardiac output that passes through the lungs without effective oxygenation.
- It requires arterial and mixed venous blood, so it is not usually calculated routinely.
Why increasing FiO₂ has limited effect in shunt
In ventilated alveoli, high FiO₂ can raise end-capillary oxygen content slightly by increasing dissolved oxygen. But haemoglobin is already almost fully saturated.
In shunt units, there is no ventilation. Blood leaves with venous oxygen content regardless of FiO₂.
When the two blood streams mix, arterial oxygen remains low if shunt fraction is large.
This is why severe shunt requires recruitment or redirection of perfusion, not just oxygen:
- PEEP or CPAP,
- recruitment manoeuvres when appropriate,
- treating pneumonia or oedema,
- drainage or relief of collapse,
- positioning,
- restoring FRC,
- treating ARDS,
- reducing shunt during one-lung ventilation.
Mixed venous oxygen and shunt
The effect of a shunt on arterial oxygenation is worse when mixed venous oxygen content is low.
Mixed venous oxygen falls when:
- cardiac output is low,
- haemoglobin is low,
- oxygen consumption is high,
- arterial oxygen content is low,
- extraction is high.
Therefore, in a patient with pneumonia or ARDS, arterial oxygenation may improve if cardiac output and haemoglobin are optimised and oxygen consumption is reduced, even if the lung lesion is unchanged.
Clinical example:
A septic patient with pneumonia may desaturate badly because they have both intrapulmonary shunt and low mixed venous oxygen content from high metabolic demand and maldistributed flow.
Quick check: shunt
What does venous admixture mean?
Reveal answer
It is mixing of deoxygenated or poorly oxygenated blood with oxygenated pulmonary venous blood, lowering arterial oxygen content.
What does the shunt equation estimate?
Reveal answer
It estimates the fraction of cardiac output passing through the lungs without effective oxygenation.
Why does low mixed venous oxygen worsen shunt hypoxaemia?
Reveal answer
The shunted blood enters the arterial mixture with even lower oxygen content, so the final arterial oxygen content falls more.
Dead Space Physiology
Definitions
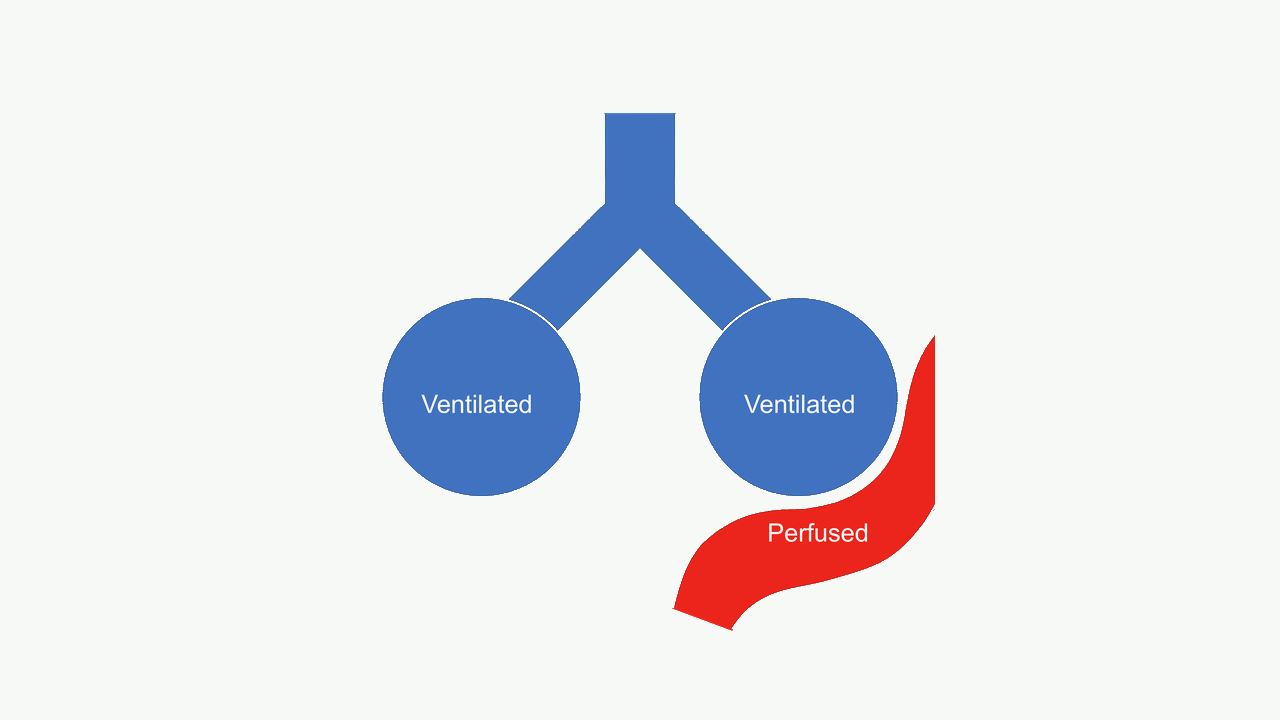
#f7f9f7; diagram labels and line work unchanged. Source link: https://commons.wikimedia.org/wiki/File:Alveolar_dead_space.png.Use this as the V/Q approaches infinity extreme: ventilation is wasted because perfusion is absent or reduced, increasing ventilatory requirement for CO2 clearance.
Dead space is ventilation that does not participate in CO₂ elimination.
Types:
| Type | Meaning |
|---|---|
| Anatomical dead space | Conducting airways that do not exchange gas |
| Alveolar dead space | Ventilated alveoli with little or no perfusion |
| Physiological dead space | Anatomical + alveolar dead space |
| Apparatus dead space | Equipment dead space between patient and circuit |
Normal anatomical dead space is approximately:
- 150 mL, or
- 2 mL/kg.
Normal physiological dead space is close to anatomical dead space in healthy lungs because alveolar dead space is small.
Bohr dead space equation
The Bohr equation estimates physiological dead space fraction:
VD/VT = (PaCO₂ − PECO₂) / PaCO₂
where:
- VD = dead space volume,
- VT = tidal volume,
- PaCO₂ = arterial CO₂,
- PECO₂ = mixed expired CO₂.
If expired CO₂ is much lower than arterial CO₂, more of the breath is dead space.
Clinical point:
End-tidal CO₂ is not the same as mixed expired CO₂, but a large PaCO₂-EtCO₂ gap often suggests increased dead space or V/Q mismatch.
Causes of increased dead space
| Cause | Mechanism |
|---|---|
| Pulmonary embolism | Ventilated alveoli lose perfusion |
| Low cardiac output | Reduced pulmonary capillary perfusion |
| Excessive PEEP | Alveolar overdistension compresses capillaries |
| Emphysema | Loss of capillary bed and alveolar walls |
| ARDS | Heterogeneous perfusion and overdistension/collapse |
| Hypovolaemia | Reduced pulmonary vascular pressure; zone 1 increases |
| Apparatus dead space | HME, connectors, long tubing near airway |
Dead space and CO₂
Dead space ventilation wastes part of each breath.
If dead space increases, the patient must increase minute ventilation to maintain PaCO₂.
Example:
A tidal volume of 500 mL with 150 mL dead space gives 350 mL alveolar ventilation per breath.
If dead space rises to 300 mL, the same tidal volume gives only 200 mL alveolar ventilation per breath.
The respiratory rate must increase substantially to maintain PaCO₂, and the work of breathing rises.
This is why pulmonary embolism, ARDS, and COPD can cause ventilatory failure.
Quick check: dead space
What makes up physiological dead space?
Reveal answer
Anatomical dead space plus alveolar dead space. Apparatus dead space adds equipment volume between the patient and circuit.
What does the Bohr equation tell you conceptually?
Reveal answer
If mixed expired CO2 is much lower than arterial CO2, more of the tidal volume is wasted as dead space.
Why does dead space increase work of breathing?
Reveal answer
More of each breath fails to eliminate CO2, so the patient must raise minute ventilation to maintain PaCO2.
Clinical Integration
Atelectasis
Atelectasis means alveolar collapse.
Physiology:
- perfusion continues,
- ventilation falls or stops,
- V/Q becomes low or zero,
- shunt increases,
- hypoxaemia develops,
- response to oxygen is limited if true collapse is extensive.
Anaesthetic causes:
- reduced FRC,
- supine positioning,
- diaphragmatic displacement,
- loss of muscle tone,
- high FiO₂ causing absorption atelectasis,
- loss of physiological glottic PEEP after intubation,
- inadequate PEEP.
Treatment principles:
- PEEP/CPAP,
- recruitment when appropriate,
- reduce excessive FiO₂ when safe,
- mobilisation,
- physiotherapy,
- treat obstruction or mucus plugging,
- adequate analgesia to allow deep breathing.
Pneumonia and consolidation
Consolidated alveoli are filled with inflammatory exudate.
Physiology:
- ventilation is poor,
- perfusion may persist,
- low V/Q or shunt develops,
- A-a gradient widens,
- oxygen response depends on how much lung is low V/Q versus true shunt.
Treatment:
- oxygen,
- antibiotics when bacterial infection suspected,
- secretion clearance,
- CPAP/PEEP or ventilation if needed,
- fluids and sepsis management when appropriate.
Pulmonary embolism
Pulmonary embolism obstructs pulmonary blood flow.
Primary physiology:
- ventilation persists but perfusion falls,
- alveolar dead space increases,
- end-tidal CO₂ may fall,
- PaCO₂-EtCO₂ gradient increases,
- hypoxaemia may occur from V/Q mismatch, low cardiac output, atelectasis, and shunt through patent foramen ovale in some patients.
Clinical signs may include:
- sudden hypoxaemia,
- tachycardia,
- hypotension if massive,
- low EtCO₂ in severe embolism,
- high dead space ventilation,
- increased pulmonary vascular resistance.
COPD and asthma
COPD and asthma cause heterogeneous airway narrowing.
Physiology:
- some units have low V/Q from poor ventilation,
- some units have high V/Q or dead space from emphysema or overinflation,
- expiratory flow limitation causes gas trapping,
- dynamic hyperinflation may increase dead space and work of breathing,
- CO₂ retention occurs when alveolar ventilation fails.
Important:
- Mild/moderate V/Q mismatch causes hypoxaemia.
- Hypercapnia suggests more severe ventilatory failure or inability to maintain minute ventilation.
ARDS
ARDS produces severe heterogeneous lung injury.
Physiology:
- alveolar flooding,
- atelectasis,
- reduced compliance,
- shunt,
- V/Q mismatch,
- increased dead space,
- pulmonary hypertension,
- impaired diffusion,
- high work of breathing.
Oxygenation may respond poorly to FiO₂ because shunt is prominent.
Treatment principles:
- lung-protective ventilation,
- appropriate PEEP,
- prone positioning in moderate/severe ARDS,
- conservative fluid strategy when appropriate,
- treat underlying cause,
- consider neuromuscular blockade, recruitment strategies, or extracorporeal support in selected severe cases.
One-lung ventilation
During one-lung ventilation:
- one lung is intentionally not ventilated,
- perfusion to that lung creates shunt,
- hypoxic pulmonary vasoconstriction reduces but does not eliminate blood flow to the non-ventilated lung,
- oxygenation depends on dependent ventilated lung function, cardiac output, shunt fraction, positioning, and anaesthetic factors.
Management principles:
- confirm tube/lung isolation position,
- optimise FiO₂,
- use appropriate PEEP to ventilated lung,
- consider CPAP to non-ventilated lung if surgical field allows,
- avoid excessive airway pressures and overdistension,
- maintain haemodynamics,
- consider effects of volatile agents on hypoxic pulmonary vasoconstriction.
Capnography and V/Q
Capnography reflects ventilation, perfusion, and metabolism.
EtCO₂ falls with:
- hyperventilation,
- reduced CO₂ production,
- low cardiac output,
- pulmonary embolism,
- increased dead space,
- disconnection or leak,
- cardiac arrest.
EtCO₂ rises with:
- hypoventilation,
- increased CO₂ production,
- rebreathing,
- malignant hyperthermia,
- return of spontaneous circulation after cardiac arrest,
- bicarbonate administration transiently in some settings.
PaCO₂-EtCO₂ gradient widens with:
- increased alveolar dead space,
- pulmonary embolism,
- low cardiac output,
- COPD/emphysema,
- ARDS,
- excessive PEEP or overdistension.
Quick check: clinical patterns
What is the dominant gas-exchange problem in atelectasis?
Reveal answer
Low V/Q or true shunt, because perfusion continues while ventilation falls or stops.
What is the dominant gas-exchange problem in pulmonary embolism?
Reveal answer
Increased alveolar dead space because ventilation persists but perfusion is reduced or absent.
Why is ARDS physiologically mixed?
Reveal answer
ARDS combines shunt, low V/Q, high dead space, diffusion impairment, reduced compliance, and high work of breathing.
High-Yield Equations and Values
Equations
How to use these equations: first classify the stem as CO2 clearance, dead space, shunt, diffusion, or V/Q matching; then choose the matching relationship.
| Equation | Meaning |
|---|---|
| CO₂ + H₂O ⇌ H₂CO₃ ⇌ H⁺ + HCO₃⁻ | CO₂ hydration and bicarbonate formation |
| PaCO₂ ∝ VCO₂ / VA | PaCO₂ depends on CO₂ production and alveolar ventilation |
| VA = RR × (VT − VD) | Alveolar ventilation |
| V/Q = alveolar ventilation / pulmonary perfusion | Ventilation-perfusion ratio |
| VD/VT = (PaCO₂ − PECO₂) / PaCO₂ | Bohr dead space equation |
| Qs/Qt = (CcO₂ − CaO₂) / (CcO₂ − CvO₂) | Shunt fraction equation |
| Diffusion ∝ A × D × ΔP / T | Fick's law concept |
| D ∝ solubility / √molecular weight | Diffusion coefficient concept |
Values to memorise
| Variable | Approximate value |
|---|---|
| PaCO₂ | 4.7–6.0 kPa / 35–45 mmHg |
| CO₂ production at rest | ~200 mL/min |
| O₂ consumption at rest | ~250 mL/min |
| Respiratory quotient | ~0.8 |
| Anatomical dead space | ~150 mL or 2 mL/kg |
| Whole-lung V/Q | ~0.8 |
| Alveolar ventilation | ~4 L/min |
| Pulmonary blood flow | ~5 L/min |
| RBC pulmonary capillary transit time at rest | ~0.75 s |
| O₂ equilibration time in healthy lung | ~0.25–0.3 s |
| Healthy alveolar-capillary membrane thickness | ~0.5–1.0 μm |
| CO₂ as bicarbonate | ~60–70% |
| CO₂ as carbamino compounds | ~20–30% |
| CO₂ dissolved | ~5–10% |
EDAIC Traps
- Most CO₂ is transported as bicarbonate, not dissolved gas.
- Bicarbonate is formed mainly inside red blood cells because carbonic anhydrase is abundant there.
- The chloride shift moves bicarbonate out of red cells and chloride into red cells in tissues.
- Deoxyhaemoglobin buffers H⁺ better than oxyhaemoglobin.
- Haldane effect: deoxygenated haemoglobin carries more CO₂.
- Bohr effect: CO₂ and H⁺ promote oxygen unloading.
- CO₂ diffuses faster than oxygen because it is much more soluble.
- Hypercapnia usually means inadequate alveolar ventilation or severe disease, not simple diffusion impairment.
- Oxygen transfer is normally perfusion-limited but can become diffusion-limited in disease or exercise at altitude.
- Carbon monoxide transfer is diffusion-limited.
- Whole-lung V/Q is about 0.8, but apex V/Q is high and base V/Q is low.
- Shunt is perfusion without ventilation: V/Q = 0.
- Dead space is ventilation without perfusion: V/Q approaches infinity.
- True shunt responds poorly to oxygen.
- V/Q mismatch usually responds to oxygen.
- Zone 1: PA > Pa > Pv; dead-space tendency.
- Zone 2: Pa > PA > Pv; flow depends on Pa − PA.
- Zone 3: Pa > Pv > PA; flow depends on Pa − Pv.
- Excessive PEEP can increase dead space by creating zone 1 conditions.
- Atelectasis causes shunt; pulmonary embolism causes dead space.
End-of-Module Summary
CO₂ is transported mainly as bicarbonate, formed inside red blood cells by carbonic anhydrase. Bicarbonate leaves the red cell in exchange for chloride, the chloride shift, while H⁺ is buffered by haemoglobin. CO₂ is also carried as carbamino compounds and in dissolved form. Dissolved CO₂ determines PaCO₂.
The Haldane effect means deoxygenated haemoglobin carries more CO₂ and buffers H⁺ better than oxygenated haemoglobin. This helps CO₂ loading in tissues and unloading in lungs. The Bohr effect is different: increased CO₂ and H⁺ reduce haemoglobin oxygen affinity and promote oxygen unloading.
PaCO₂ is mainly determined by CO₂ production divided by alveolar ventilation. Alveolar ventilation is respiratory rate times tidal volume minus dead space. Hypercapnia usually means inadequate alveolar ventilation, increased CO₂ production, increased dead space, or severe lung disease.
Diffusion follows Fick's law. It improves with large surface area, thin membrane, large pressure gradient, high solubility, and low molecular weight. CO₂ diffuses faster than oxygen because it is much more soluble. Oxygen transfer is normally perfusion-limited but can become diffusion-limited in disease or extreme conditions. Carbon monoxide transfer is diffusion-limited and is used to measure DLCO.
V/Q ratio is alveolar ventilation divided by perfusion. The average whole-lung ratio is about 0.8. In the upright lung, V/Q is high at the apex and low at the base. Shunt means perfusion without ventilation, V/Q = 0. Dead space means ventilation without perfusion, V/Q tends to infinity.
West zones describe pulmonary blood flow using alveolar, arterial, and venous pressures. Zone 1 is PA > Pa > Pv and represents dead space. Zone 2 is Pa > PA > Pv and flow depends on Pa − PA. Zone 3 is Pa > Pv > PA and flow depends on Pa − Pv.
Hypoxaemia results from low inspired oxygen, hypoventilation, diffusion impairment, V/Q mismatch, or shunt. V/Q mismatch usually improves with oxygen. True shunt responds poorly because shunted blood does not contact alveolar gas.
The key message is:
When gas exchange fails, identify whether the problem is ventilation, perfusion, diffusion, shunt, dead space, or CO₂ production. The treatment depends on the failed step.